1Department of Pharmacy, Faculty of Allied Health Sciences, University of Peradeniya, Sri Lanka.
2Department of Nursing, Faculty of Allied Health Sciences, University of Peradeniya, Sri Lanka.
TMIUK Tennakoon
Email: imalka@ahs.pdn.ac.lk
Received : Dec 09, 2024 Accepted : Jan 15, 2025 Published : Jan 22, 2025 Archived : www.meddiscoveries.org
Objectives: To determine the association between health literacy, subjective well-being, and knowledge about dietary supplements and dietary supplement intake among the staff members at the University of Peradeniya, Sri Lanka.
Design: Descriptive cross-sectional study using a pre-tested and validated questionnaire.
Setting and participants: 355 academic and non-academic staff members attached to the University of Peradeniya, Sri Lanka.
Results: Participants’ prevalence rate of dietary supplements was 74.3%. The mean values of health literacy, subjective well-being, and knowledge about dietary supplements were 34.09±6.55, 15.06±5.74, and 12.64±2.11, respectively. For all participants, nutritional information on the package was the most considerable factor when choosing a dietary supplement, followed by price. The most common reason for taking dietary supplements was to promote general health, followed by a recommendation from medical officers. Dietary supplement intake was significantly associated with the staff members’ education level (p=0.021) and subjective well-being (p=0.006).
Conclusion: The current use of dietary supplements among the university staff is at a moderate level. Academic staff members have more subjective well-being, health literacy, and knowledge about dietary supplements compared to non-academic staff members. This study recommends the implementation of awareness programs on dietary supplements for the University population.
Keywords: Dietary supplements; Subjective well-being; Health literacy; Knowledge; University staff.
Dietary Supplements (DS) are products, which contain dietary ingredients and are intended to ingest into the body. Dietary ingredients are a combination of a vitamin, a mineral, a herb or other botanical, and amino acids [1-3]. The primary goals of DS are to promote general health, enhance sports performance, treat specific diseases, and improve performance and energy and doctor’s recommendation [15]. Dietary supplements are available as tablets, capsules, powders, soft gels, gel caps, or liquid [2,4-6]. They consist of fillers, binders, and several flavors other than dietary ingredients. Food and Drug Administration, USA (FDA) regulates DS as food, not as a drug and as such dietary supplements are available in pharmacies and other groceries, and online stores [7] while most of these products can be bought without a prescription [6-8]. DS can be used with or without conventional medicines [9]. However, DS can alter the absorption, metabolism, and disposition of conventional medicines [2].
People in both developed and developing countries use dietary supplements [4,12]. In developed countries, ≥75% of the population uses DS. Previous studies have reported that dietary supplements, which were designed to supplement the diet with additional nutrients, have grown in popularity around the world [13]. In the past few years, the consumption rate of dietary supplements has increased consistently. For various nations, prevalence data on the general public’s frequent use of dietary supplements during the last few decades are available however data is not available in the Sri Lankan setting [14].
Specific therapeutic purposes or general health and well-being are the major purposes of the consumption of dietary supplements [6]. However dietary supplements cannot replace healthy foods [15]. The Degree of consumption of dietary supplements has been shown to be associated with various factors such as education, race, ethnicity, gender, age, physical activity, disease state and income [4,13,16].
Sriratai et al (2021) revealed that consumption of DS is linked to age and health literacy [17]. Health literacy can be defined as an ability to achieve, operate and realize the fundamental information and services to make suitable health decisions. Wide understanding ability and ability to process or perform mathematical concepts affect the health literacy of the patient. Healthy Eating Index (HEI-2005) investigates the relationship between health literacy and diet quality (food choices and degree of nutrient intake), which shows positive results [18].
There is also a relationship between the subjective well-being and intake of DS. Subjective well-being can be described using different aspects, which are physical well-being, recreation, and social activities. Good health is needed for maintaining physical well-being and majority of the people take DS to improve their good health by maintaining a balanced diet [20,22].
Although DS is essential for maintaining good health, there are several risk factors associated with DS such as not enough evidence-based research on the safety and efficacy of DS and potential dietary supplement-drug interactions [11], contradictory and confusing information from mass media [12], limited information availability on pattern of use, reason of use, and amount of use [15], the use of different DS at the same time [7], inappropriate use of DS [7,8] and dietary ingredients having a significant impact on the body (e.g. Heavy metals, undeclared allergens or illegal drug). The most common adverse events include nausea, vomiting, diarrhea, cardiovascular complications, anxiety, fever and liver injury [3,10]. Therefore, it’s clear that public awareness regarding DS is important.
Sri Lanka is a developing country. Compared to the developed countries, less percentage of the population use DS in Sri Lanka. Limited availability, poor financial status and lack of knowledge about DS are the major causes [27]. Dietary supplements are classified as “borderline products” under the National Medicines Regulatory Authority (NMRA – Sri Lanka) Act of 2015, which defines them as items with combination characteristics of medicines and foods. In Sri Lanka, compared to other countries, laws governing the import and sale of nutritional supplements are less strict than conventional medications. The primary health issue in Sri Lanka has been malnutrition, but the recent advent of the obesity pandemic has resulted in a plethora of weight-loss supplements in the market [28]. The university population is more vulnerable to nutritional deficiencies. Their studies, activities, alcohol consumption and smoking can be considered as common causes of nutritional deficiencies [5]. Therefore, dietary supplements are widely popular among university population [5,12]. They use DS for relieving stress and improving their health conditions. Some university students also follow their own diet plan to improve their lifestyle characteristics [12]. This study was carried out to determine the association between health literacy, subjective well-being, knowledge about dietary supplements and dietary supplements intake in a Sri Lankan university population to fill the current knowledge gap in this area.
Study participants
This was a descriptive cross-sectional study conducted at the University of Peradeniya, Sri Lanka. The sample size was 355 (190 academic staff members and 165 non-academic staff members|). All academic and non-academic staff members of the University were included while the staff members who were on leave during the data collection period were excluded. Before the data collection process, ethical approval was obtained from the Ethics Review Committee at the Faculty of Allied Health Sciences, University of Peradeniya. A pre-test was performed to validate the questionnaire. Out of the 355 staff members who were asked to participate in the study only 120 academic staff members (63.13%) and 165 non-academic staff members (84.84%) consented to participate in the study.
Measurements
The questionnaire consisted of five sections. The first section consisted of sociodemographic factors of study participants including age, sex, height, weight, monthly income, and education level.
The second part consisted of the consumption of dietary supplements while the third part consisted of the subjective well-being of the participants. It contained 5 questions. The following scale was used to rate the answers of all respondents. All the time=5, most of the time=4, more than half of the time=3, less than half of the time=2, some of the time=1, at no time=0. The total raw score, ranging from 0 to 25, is multiplied by 4 to give the final score, with 0 representing the worst imaginable well-being and 100 representing the best imaginable well-being.
The fourth part measured the health literacy of all participants. It consisted of 12 questions. All responses were measured using the following scale. 4=very easy, 3=fairly easy, 2=fairly difficult, 1=very difficult. The fifth part measured the knowledge about dietary supplements. The responses were rated as, 1=true, 0=false.
Paper based questionnaire was distributed to the non-academic staff members and a google form was distributed among the academic staff members. Paper based questionnaire consisted of Sinhala, English and Tamil medium while google form consisted of only English medium. Previously validated questionnaire was used under the permission of original authors.
Statistical analysis
The data was analyzed using descriptive statistical analysis, chi-square test, independent t-test, and hierarchical regression analysis. To gain a basic picture of the respondents, descriptive statistical analysis was used to determine demographic variables, health literacy, subjective well-being, and dietary supplement usage. Two regression models were created to investigate the impact of demographic characteristics (such as age, gender, financial status, education level and BMI) on dietary supplement intake, as well as subjective-well-being and health literacy and knowledge.
Sociodemographic factors
The response rate was 70.14%. The total number of responses of non-academic staff was 140 (84.84%) and the academic staff was 120 (63.15%) (Table 1).
The mean age of the total sample is 39.71±9.98 yrs. More than half of the respondents were females, 140 (56.2%) followed by males, 109 (43.8%). Most of the sample was within the normal weight 141 (56.6%) followed by obese 94 (37.8%) and underweight category 14 (5.6%). The mean income of the population was 101290.34±99843.31 LKR. Most of the 46 (18.5%), Ph.D. 32 (12.9%), undergraduate 14 (5.6%), MSc 14 (5.6%), and primary education 4 (1.6%) (Table 1).
The consumption of dietary supplements
The knowledge of the participants with regards to dietary supplements is summarized in Table 2.
Most of the participants take dietary supplements to promote their general health (45.4%), followed by recommendations from medical officers (34.5%), specific nutritional and health promotion (26.9%), recommendations from others (25.3%), friends taking dietary supplements (17.3%), no reason (14.5%) and other reasons (5.6%).
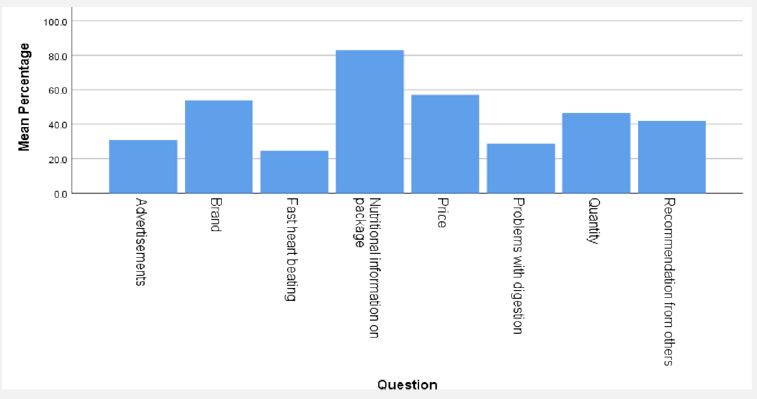
The factors that are considered during the consumption of dietary supplements are shown in Figure 1. Most of the participants consider nutritional information on the package (83.5%) followed by price (58.2%), brand (55.4%), quantity (47.0%), recommendation from others (42.6%), advertisements (31.3%), problems with digestion (28.9%), and fast heart beating (23.7%) during consumption.
The subjective well-being of the participants
The subjective well-being of the participants is summarized in Table 3.
The health literacy
The health literacy of the participants is summarized in Table 4.
The association between dietary supplements intake with health literacy, subjective well-being and knowledge about dietary supplements
The association between dietary supplement intake with subjective well-being, health literacy and knowledge were analyzed using regression. The mean value of the subjective well-being is 15.06±5.748. The mean value of health literacy of the total sample is 34.09±6.554. The mean value of the knowledge is 12.64±2.115. Among these independent variables, only subjective well-being (p=0.006) was significantly associated with dietary supplement intake. Health literacy (p=0.267) and knowledge (p=1.154) do not show any significant association with dietary supplement consumption.
When analyzing the association between the dietary supplement intake and the sociodemographic factors age (p=0.076), gender (p=0.996), BMI level (p=0.064), and income did not show any association with dietary supplement intake. Education level (p=0.021) is significantly associated with the intake of dietary supplements.
| Factor | Mean | SD | Frequency | Percentage | |
|---|---|---|---|---|---|
| Age | 39.71 | 9.98 | |||
| Gender | Female | 140 | 56.2 | ||
| Male | 109 | 43.8 | |||
| BMI level | Underweight | 14 | 5.6 | ||
| Normal weight | 141 | 56.6 | |||
| Obese | 94 | 37.8 | |||
| Income | 101290.34 | 99843.31 | |||
| Education level | Primaryeducation | 4 | 1.6 | ||
| Secondary education | 53 | 21.3 | |||
| Diploma | 46 | 18.5 | |||
| Undergraduate | 14 | 5.6 | |||
| Graduate | 63 | 25.3 | |||
| Msc | 14 | 5.6 | |||
| MPhil | 22 | 8.8 | |||
| PhD | 32 | 12.9 | |||
| Question | Yes | No |
|---|---|---|
| Taking vitamin and mineral supplements prevents diseases in healthy patients | 201 (80.7) | 48 (19.3) |
| The quality of dietary supplements is routinely testedbefore being marketed | 173 (69.5) | 76 (30.5) |
| People with kidney diseases should not usehigh doses of vitamin C | 149 (59.8) | 99 (39.8) |
| The use of multivitamin preparations protects againstheart diseases | 135 (54.2) | 114 (45.8) |
| An ingredient may be soldboth as a medicine or as a dietary supplement | 146 (58.6) | 103 (41.4) |
| Taking excessive amounts of magnesium supplements can causediarrhea and nausea | 210 (84.3) | 39 (15.7) |
| Before beingmarketed, dietary supplements must be testedfor efficacy andsafety | 198 (79.5) | 51 (20.5) |
| In the elderly, the use of magnesium preparations prevents muscle cramps | 144 (57.8) | 105 (42.2) |
| The packaging of dietary supplements must contain information on possible adverse effects resulting fromtheir use | 136 (54.6) | 113 (45.4) |
| Dietary supplements are food | 136 (54.6) | 113 (45.4) |
| Taking dietarysupplements containing Calciumreduces the risk of bonefractures in theelderly | 229 (92.0) | 20 (8.0) |
| Dietary supplement registration requires assessing the composition of the product by the appropriate supervisory body | 163 (65.5) | 86 (34.5) |
| The use of antioxidants prevents the development of cancer | 164 (65.9) | 85 (34.1) |
| In the elderly, takingvitamin D reducesthe risk of bone fractures | 189 (75.9) | 60 (24.1) |
| Vitamin C naturally present in food is better assimilated than synthetic | 103 (41.4) | 146 (58.6) |
| All dietarysupplements sold in pharmacies havebeen tested forsafety | 152 (61.0) | 97 (3.0) |
| Regular use of vitamin C reduces the risk of catching a cold | 150 (60.8) | 99 (39.2) |
| Questions | Responses | |||||
|---|---|---|---|---|---|---|
| All the time | Most of the time | More than halfof the time | Less than halfof the time | Some of the time | At no time | |
| I havefelt cheerful and in good spirits | 41 (16.5) | 89 (35.7) | 46 (18.5) | 20 (8.0) | 38 (15.3) | 15 (6.0) |
| I havefelt calm andrelaxed | 28 (11.2) | 79 (31.7) | 39 (15.7) | 32 (12.9) | 54 (21.7) | 17 (6.8) |
| I havefelt active andvigorous | 34 (13.7) | 104 (41.8) | 44 (17.7) | 29 (11.6) | 29 (11.6) | 7 (2.8) |
| I wokeup feeling freshand relaxed | 34 (13.7) | 96 (38.6) | 40 (16.1) | 34 (13.7) | 33 (13.3) | 11 (4.4) |
| My dailylife has beenfilled with thingsthat interest me | 25 (10.0) | 56 (22.5) | 61 (24.5) | 33 (13.3) | 61 (24.5) | 13 (5.2) |
Question |
Responses |
|||
|---|---|---|---|---|
| Very easy | Fairly easy | Fairlydifficult | Verydifficult | |
| Find information on treatments of illnesses thatconcern you? | 46 (18.5) | 162 (65.1) | 31 (12.4) | 7 (2.8) |
| Understand theleaflets that comewith your medicine? | 42 (16.9) | 149 (59.8) | 41 (16.5) | 16 (6.4) |
| Judge theadvantages and disadvantages of different treatment options? | 19 (7.6) | 123 (49.4) | 84 (33.7) | 21 (8.4) |
| Call an ambulance in an emergency? | 90 (36.1) | 96 (38.6) | 45 (18.1) | 12 (4.8) |
| Find information on how to manage mentalhealth problems likestress or depression? | 43 (17.3) | 114 (45.8) | 74 (29.7) | 16 (6.4) |
| Understand why you needhealth screenings (suchas breast exam,blood sugar test,blood pressure)? | 79 (31.7) | 119 (47.8) | 39 (15.7) | 10 (4.0) |
| Judge whichvaccinations you may need? | 37 (14.9) | 81 (32.5) | 82 (32.9) | 45 (18.1) |
| Decide how you can protect yourself from illness basedon advice fromfamily and friends? | 71 (28.5) | 117 (47.0) | 43 (17.3) | 15 (6.0) |
| Findout about activities (such as meditation, exercise, walking, Pilates etc.) that aregood for yourmental-well-being? | 80 (32.1) | 127 (51.0) | 28 (11.2) | 12 (4.8) |
| Understand information in the media(such as theinternet, newspaper, magazines) on how to get healthier? | 110 (44.2) | 112 (45.0) | 20 (8.0) | 5 (2.0) |
| Judge whicheveryday behavior (suchas drinking and eating habits,exercise etc.) is related to your health? | 100 (40.2) | 111 (44.6) | 29 (11.6) | 6 (2.4) |
| Join a sports clubor exercise classif you wantto? | 73 (29.3) | 83 (33.3) | 60 (24.1) | 30 (12.0) |
This study was designed to determine the association between the health literacy, subjective well-being, knowledge, and intake of dietary supplements among staff members of University of Peradeniya Sri Lanka. The highest number of participants belonged to the non-academic staff. More than half of the total participants were females. These results represent the general demographic information of the Sri Lankan university employees.
Mean age of the participants was 39.71±9.98 yrs. Age is a factor in the prevalence of supplement use among academic staff in the current investigation. Because academic staff members have more scientific knowledge and they have more interaction with social media than the non-academic staff members and academic staff members are more up to date than non-academic staff members [4].
In our study, gender does not affect the intake of dietary supplements [14]. Most of the participants were in the normal weight category (56.6%). Previous studies have indicated that gender does not affect the intake of dietary supplements [5,16]. But developed countries indicated that both gender and age were affecting the intake of dietary supplements [14]. There is a correlation with BMI level and consumption of dietary supplements. But there was no significant association between the BMI level and dietary supplements consumption in the current study. It may be due to the non-linear relationship between BMI and DS consumption. But a previous study by Zezelj et. Al., revealed that dietary supplements consumption was significantly associated with BMI level [5].
Mean income of the total participants was 101290± 99843. .31 LKR. Tsartsou et al, 2021 revealed that dietary supplements intake is significantly associated with income. However, our study does not show that association.
Most of the participants had their maximum education level up to graduates. There was a significant association between DS intake and education level. A previous study by Barnes et al., in 2016 also showed that education is significantly associated with dietary supplements usage [4].
To our knowledge, this is the first study in Sri Lanka to document dietary supplement use in the University population. Dietary supplementation is a worldwide practice throughout the world, in both developed and developing countries. Among the total sample, the prevalence of dietary supplement usage is 74.3%. Majority of participants used dietary supplements at least once. 44.6% of the sample are currently using dietary supplements. But it is lower than the prevalence rate of other developed and developing countries4.
The mean value of the subjective well-being was above the reference [13] of both samples [32]. Therefore, both academic and non-academic staff members have good subjective well-being. Also, it significantly associated with the consumption of dietary supplements of the academic staff members.
Comparing the mean values of the health literacy in academic and non-academic staff, academic staff members have more health literacy than the non-academic staff members. But it is not significantly associated with dietary supplements consumption. But a previous study by District et. Al., in 2021 revealed that there was a significant association between health literacy and DS consumption [17].
According to our results academic staff members have more knowledge about dietary supplements than the non-academic staff. But there is no association of health literacy and knowledge of dietary supplements with consumption of dietary supplements. However, a previous study kolodiziej et. al., indicated that there was a significant association between DS intake and knowledge about DS [7].
Among the reasons for consumption of dietary supplements most of the participants took dietary supplements to promote their general health, followed by recommendation from medical officers, specific nutritional and health promotion, recommendation from others, friends taking dietary supplements, no reason and other reasons. Most of the participants considered factors such as, nutritional information on the package followed by price, brand, quantity, recommendation from others, advertisements, problems with digestion, and fast heart beating when they were buying the supplements. A previous study by Choi et. al., in 2029 reported that nutritional information is the most important factor among the participants [12].
Among the dietary supplement’s users of non-academic staff, most of them did not have a proper idea about the meaning of the dietary supplements. This may indicate that many people who use dietary supplements believe them to be beneficial yet are unsure of how they affect their body systems [4].
There were certain variations where the uses of certain dietary supplements closely matched their indications. An individual’s motivation for using a dietary supplement may be influenced by its perceived effectiveness. The results of this study showed that, more than half of the participants had no proper idea about the meaning of the dietary supplements. Higher levels of education and knowledge about dietary supplements also significantly influence their trust, and eventually their choice to buy this class of goods [4]. In addition, those with higher income and education levels are more conscious of dietary supplements than people with lower income and education level [34].
It is concluded that the prevalence rate of current use of dietary supplements is at a moderate level. Academic staff members have more subjective well-being, health literacy, and knowledge about dietary supplements compared to non-academic staff members. Dietary supplement intake is significantly associated with education level and subjective well-being. Many of the staff members consider nutritional information on the package rather than the price of the product. General health promotion is the main purpose of consumption of DS.
Based on the results, it is recommended that awareness programs on dietary supplements should be implemented for the University population to increase their knowledge.
Strengths and limitations of this Study
− This is the first study conducted in Sri Lanka with the University population as a study sample.
− The study sample is restricted to only one university, so it does not represent the whole university population in Sri Lanka.
Funding statement: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: All authors declare no competing interests.
Author contribution: DM and TM conceptualized the study, designed the methodology, analyzed the data, supervised, and revived the manuscript. MS carried out the investigation, wrote the original draft and reviewed the manuscript.
