1Department of Hepato-Gastroenterology & Internal Medicine, University Clinics of Kinshasa, DR Congo.
2Department of Infectious and Tropical Diseases/Tropical Medicine & Internal Medicine, University Clinics of Kinshasa, DR Congo.
3Department of Faculty of Medicine, University of Kikwit, DR Congo.
4Department of Faculty of Veterinary Medicine, University of Montreal, Canada.
5Department of Social and Preventive Medicine, School of Public Health, University of Montreal, Canada.
6Department of Cardiology & Internal Medicine, University Clinics of Kinshasa, DR Congo.
7Department of Pathological Anatomy, University Clinics of Kinshasa, DR Congo.
8School of Public Health of Kinshasa, DR Congo.
Pauline Phaka Bikuelo
Email: youyou.phaka@gmail.com
Received : Feb 03, 2025 Accepted : Mar 07, 2025 Published : Mar 14, 2025 Archived : www.meddiscoveries.org
Background: Anorectal Lesions (ARL) are common in people living with HIV (PLWH). The aim of this study was to describe the frequency and the clinico-endoscopic and histopathological aspects of ARL in PLWH who presented with proctological complaints.
Methods: Descriptive cross-sectional study that included any PLWH aged at least 18 years, with at least one proctological complaint, and followed up on an outpatient or inpatient basis at the Department of Internal Medicine of the University of Kinshasa Hospital and at the ACS/Amo-Congo (Action Communautaire contre le SIDA/Avenir Meilleur pour les Orphelins du SIDA au Congo) center in Kinshasa/Kasa-vubu between April 1, 2011, and January 31, 2012. Sociodemographic, clinical, biological and therapeutic data were collected. Anorectal endoscopy was performed and biopsy specimens for anatomopathological examination were taken.
Results: Overall, 168 PLWH [mean age (SD): 45.2 years (9.4 years); 74% female] were included in the study. One hundred and twenty patients (71.4%) presented with at least one ARL. Anal tumefaction (57.7%) and anal pruritus (35.1%) were the most commonly reported proctological complaints. Hemorrhoidal disease (60.8%) and anal fissure (24.2%) were the most frequently diagnosed ARL in patients. Histopathological analysis of biopsies confirmed 3 cases of condyloma acuminata and two cases of anal cancer, one infiltrating well-differentiated mucoepidermoid carcinoma and one invasive well-differentiated squamous cell carcinoma.
Conclusion: In PLWH with proctological symptoms, ARL are common and should be systematically investigated for early diagnosis and appropriate management.
Keywords: Anorectal lesion; Anal pathology; HIV; Kinshasa.
According to World Health Organization (WHO) statistics, 39.0 million (33.1-45.7 million) people were living with Human Immunodeficiency Virus (HIV) at the end of 2022, more than two-thirds (25.6 million) of whom were in the WHO African Region [1]. In the same year, the number of people who died from HIV was 630,000 (480,000-880,000), and 1.3 million (1.0-1.7 million) people acquired HIV [1]. The prevalence of HIV infection in the Democratic Republic of Congo (DR Congo) is estimated at 1.2% in the general population aged 15-49 years and 2.77% in pregnant women aged 15-49 years [2]. HIV infection can affect multiple organs and systems due to the effect of the virus itself or its effects on the immune system [3-5]. The manifestations of organ damage during HIV infection are therefore variable and appear to be closely linked to the degree of immunosuppression [6-9]. At the digestive level, esophageal disorders, gastric disorders, enteritis, diarrhea, colitis and anorectal pathology are among the most common gastrointestinal manifestations documented in HIV [10].
Anorectal pathology is the most common surgical condition in patients with HIV and Acquired Immunodeficiency Syndrome (AIDS) [11]. Anorectal lesions (LAR) are more common in patients with HIV/AIDS than in the general population [11,12]. In PLWH, LARs are explained both by the immunological alterations produced by HIV and by other risk factors, in particular the practice of anal intercourse [5,11]. They are quite common in PLWH with collapsed CD4 lymphocyte counts [13], and a considerable immunodeficiency can promote more serious and prolonged lesions [13,14].
The prevalence of anorectal diseases varies between studies and populations examined. In Chile, Muñoz et al. [11] reported a prevalence of LAR of 13% in PLWH admitted to the infectious disease’s unit of a reference hospital, with a predominance of anal condylomas and hemorrhoids. In France, a study of PLWH on triple ARV therapy and followed up in the infectious diseases unit of a Parisian hospital showed that 44% of these patients had at least one macroscopic LAR [15], suggesting that anorectal pathology remains prevalent and has not been substantially modified by the advent of ARV therapy [5,16,17]. In sub-Saharan Africa, studies on LAR during HIV infection are relatively rare and practically nonexistent in the DR Congo. The aim of the present study was to describe the frequency and clinico-endoscopic and histopathological aspects of LAR in PVV with proctological complaints.
Type, setting and period of the study
This is a descriptive cross-sectional study that included PLWH followed at the Department of Internal Medicine of the University Clinics of Kinshasa (CUK) and at the ACS/Amo-Congo center (Community Action against AIDS/Avenir Meilleur pour les Orphelins du SIDA au Congo) in the city of Kinshasa, DR Congo. These two structures are approved for the care of PLWH by the National AIDS Control Program (PNLS) in DR Congo. The study took place between April 1, 2011 and January 31, 2012.
Study population
The target population of the study was adult patients living with HIV, followed at CUK and ACS/AMO-Congo and with proctological complaints. Eligible for the study were any confirmed PLWH aged at least 18 years, followed in outpatient consulta consultation or admitted to hospital in the medical facilities previously identified during the study period, who had at least one proctological complaint. Any patient whose medical record contained positive results of the anti-HIV 1-2 Elisa serology or at least two rapid tests using two different principles was considered a confirmed PLWH. We excluded PLWH in whom it was not possible to perform anorectal endoscopic examination (medical reasons or patient refusal) and those who did not consent to participate in the study. Patient recruitment was consecutive and any patient who met all the eligibility criteria and who did not meet any exclusion criteria was included in the study.
Data collection
Data collection was carried out in four stages: patient interview, review of their medical records, general physical and proctological examination, and anatomopathological analysis of samples taken from a few LARs. Data collection was carried out by a team of trained investigators. The interview with the patient took place in a consultation room in each of the two medical training courses. Sociodemographic characteristics (age, sex, marital status, level of education), the year of discovery of HIV seropositivity, proctological complaints and the patient’s medical history were collected.
We defined duration of HIV seropositivity as the difference between the date of the survey and the date of discovery of HIV seropositivity. The medical records of each eligible patient were reviewed by the investigators to collect data on comorbidities, clinical stage of HIV infection according to the WHO classification [18], CD4 lymphocyte count and the antiretroviral treatment regimen applied. Comorbidities and clinical stage of HIV infection according to the WHO were recorded as reported in the patient’s medical records. The CD4 count considered was that dating back less than three months from the date of the survey. It was dichotomized at the threshold of 200 cells/mm3, below which immunodeficiency is considered severe [18].
The physical examination was performed in the same consultation room. Systolic Blood Pressure (SBP, mm Hg) and Diastolic Blood Pressure (DBP, mm Hg) were measured using an electronic sphygmomanometer in a sitting position and at rest for at least 5 minutes. Weight and height were measured in a standing position, barefoot and lightly dressed, using, respectively, a wall-mounted height rod and a SECA scale. Body Mass Index (BMI) was calculated as the ratio of weight (kg) to the square of height (m²). The proctological examination was performed in the gastroenterology department of the CUK under the supervision of two gastroenterologists and a senior assistant physician in gastroenterology. The examination began with an anoperineal visual inspection, followed by a digital rectal examination, then anoscopy and rectoscopy. Anoscopy was performed with an anoscope connected to a cold light source. Rectoscopy was performed with rigid equipment. Biopsy samples for histopathological analysis were taken from some tumor-like lesions detected.
Data analysis
Data processing and analysis were performed using STATA/MP software version 17.0 (StataCorp, Texas, USA) and Microsoft Excel© 2016. Qualitative variables were described as absolute frequency (n) and/or percentage. Continuous quantitative variables were described by the mean with standard deviation or median with extreme values depending on whether their distribution was symmetrical or not, respectively. Pearson’s Chi-square test was used for contingency table analysis. Student’s t-test and Wilcoxon/Mann-Whitney non-parametric test were applied to compare means and medians by gender or presence of LAR, respectively. The value of p<0.05 was the threshold for statistical significance.
Ethical considerations
All participants provided free, informed and written consent before participating in the study. Patient data were de-identified to ensure confidentiality of information and preserve patient dignity. The protocol of this study was approved by the Department of Internal Medicine of CUK.
General characteristics of PLWH in the present study
A total of 168 PLWH were included in the study, including 143(85%) at the Amo-Congo site and 25(15%) at the CUK, with a predominance of females (74%). Table 1 describes the sociodemographic characteristics of PLWH according to their gender. The patients had a mean age of 45.2 years, 41.7% were married, predominantly men than women (65.9% vs. 33.1%, overall p-value=0.001). Approximately eight out of 10 patients (79.8%) had completed secondary or vocational education. On the professional level, 47% and 35.1% of patients, predominantly women, were unemployed and self-employed, respectively.
Frequency of LAR
In total, 120 of the 168 PLWH were carriers of LAR, representing a frequency of LAR of 71.4%. The frequency of LAR did not differ significantly by sex (81.8% in men versus 67.7% in women; p=0.076).
Clinical, biological and therapeutic profile of PLWH
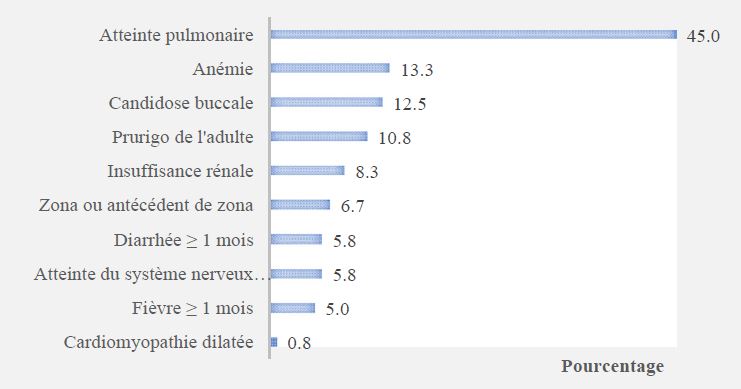
Table 2 presents the clinical, biological and therapeutic characteristics of patients according to the presence of LAR. The median duration of anti-HIV seropositivity was 44 months, with no significant difference between groups. The most reported proctological complaints were anal swelling (57.7%), anal pruritus (35.1%) and anorectal pain (23.8%), with no significant differences between groups. Constipation was statistically significantly more reported by patients with LAR compared to others (27.5% vs. 4.2%; p=0.001). Hematochezia and purulent discharge were exclusively reported by patients with LAR. In total, 80.4% of patients were clinically WHO stages 3 and 4. SBP, DBP and BMI did not differ significantly between groups. Pulmonary involvement was the most documented comorbidity in patients with LAR (Figure 1). The median CD4 lymphocyte count was statistically significantly higher in patients with LAR than in those without (300 cells/mm3 vs. 193 cells/mm3; p=0.016). Overall, 87.5% of PLWH were treated with ARVs, with the combination of stavudine + lamivudine + nevirapine or efavirenz being prescribed in 81.7% of all patients, with no significant difference according to LAR (Table 2).
Anorectal clinico-endoscopic lesions in PLWH
The frequency of anorectal clinical and endoscopic lesions is presented in (Table 3). Hemorrhoidal disease (60.3%) and anal fissure (24.2%) were the most frequently encountered LARs in patients.
Anatomopathological aspects of some LAR
Biopsy samples were taken from 5 patients with LAR (three cases of condylomata acuminata and two cases of budding anal mass) and were subjected to anatomopathological analysis. Condylomata acuminata were confirmed for all three patients, while the findings for the two cases of budding anal masses were, respectively, a well-differentiated infiltrating mucoepidermoid carcinoma (or adenosquamous carcinoma) and an invasive well-differentiated squamous cell carcinoma.
| Caractéristiques | Tous (n=168) | Masculin (n=44) | Féminin (n=124) | p |
|---|---|---|---|---|
| Age, years, mean±SD | 45,2±9,4 | 47,3±9,7 | 44,5±9,2 | 0,086 |
| Marital status, n (%) | 0,001 | |||
| Single | 38(22,6) | 7(15,9) | 31(25,0) | |
| Divorced | 14(8,3) | 4(9,1) | 10(8,1) | |
| Married | 70(41,7) | 29(65,9) | 41(33,1) | |
| Widowed | 46(27,4) | 4(9,1) | 42(33,8) | |
| Education level, n (%) | 0,226 | |||
| Primary or noeducation | 8(4,8) | 1(2,3) | 7(5,6) | |
| Secondary or vocational | 134(79,8) | 33(75,0) | 101(81,5) | |
| University | 26(15,4) | 10(22,7) | 16(12,9) | |
| Occupation, n (%) | <0,001 | |||
| Unemployed | 79(47,0) | 13(29,6) | 66(53,2) | |
| Students | 1(0,6) | 0(0,0) | 1(0,8) | |
| Self-employed | 59(35,1) | 13(29,6) | 46(37,1) | |
| Employees | 29(17,3) | 18(40,8) | 11(8,9) |
Abbreviations: HIV: Human Immunodeficiency Virus; SD: Standard Deviation.
| Tous (n=168) | Pasde LAR (n=48) | Avec LAR (n=120) | p | |
|---|---|---|---|---|
| Clinical features | ||||
| Duration of HIV seropositivity, months,med (range) | 44(1–264) | 47(5–264) | 43(1–138) | 0,109 |
| Anal swelling, n (%) | 97(57,7) | 24(50,0) | 73(60,8) | 0,199 |
| Anal pruritus, n (%) | 59(35,1) | 20(41,7) | 39(32,5) | 0,261 |
| Anorectal pain, n (%) | 40(23,8) | 7(14,6) | 33(27,5) | 0,076 |
| Constipation, n (%) | 35(20,8) | 2(4,2) | 33(27,5) | 0,001 |
| Hematochesis, n (%) | 17(10,1) | 0(0,0) | 17(14,2) | - |
| Purulent discharge, n(%) | 8(4,8) | 0(0,0) | 8(6,7) | - |
| WHO clinical stage,n (%) | 0,299 | |||
| I | 10(5,9) | 5(10,4) | 5(4,2) | |
| II | 23(13,7) | 8(16,7) | 15(12,5) | |
| III | 110(65,5) | 30(62,5) | 80(66,6) | |
| IV | 25(14,9) | 5(10,4) | 20(16,7) | |
| SBP, mm Hg, mean ±SD | 109±11 | 109±10 | 109±11 | 0,919 |
| DBP, mm Hg, mean ±SD | 67±9 | 67±8 | 68±9 | 0,566 |
| BMI, kg/m2,mean ± SD | 22,2±4,8 | 21,6±5,0 | 22,4±4,8 | 0,342 |
| Laboratory features | ||||
| CD4 count, cells/mm3, med (range) | 267(1-1150) | 193(1-1150) | 300(2-1090) | 0,016 |
| <200, n (%) | 57(33,9) | 25(52,1) | 32(26,7) | 0,002 |
| ≥200, n (%) | 111(66,1) | 23(47,9) | 88(73,3) | |
| Therapeutic features | ||||
| ARV treatment regimens | 0.177 | |||
| No treatment | 21(12,5) | 9(18,8) | 12(10,0) | |
| D4T+3TC+NVP ou EFV | 131(78,0) | 33(68,7) | 98(81,7) | |
| DDI+ABC+LP/r | 16(9,5) | 6(12,5) | 10(8,3) |
| Anorectal lesions | n/120 | % |
|---|---|---|
| Hemorrhoidal disease | 73 | 60,8 |
| Anal fissure | 29 | 24,2 |
| Marisque | 16 | 13,3 |
| Anal mycosis | 14 | 11,7 |
| Anal ulceration | 11 | 9,2 |
| Proctitis appearance | 6 | 5,0 |
| Anal abscess | 5 | 4,2 |
| Anal herpes | 4 | 3,3 |
| Condyloma acuminatum | 3 | 2,5 |
| Anitis appearance | 3 | 2,5 |
| Budding anal mass | 2 | 1,7 |
| Anal fistula | 1 | 0,8 |
LARs are one of the most common gastrointestinal manifestations in PLWH [10]. The present study, conducted on a group of PLWH presenting with proctological symptoms at the CUK and the ACS/Amo-Congo center in Kinshasa, aimed to describe the frequency and the clinico-endoscopic and histopathologihistopathological aspects of LARs in PLWH with proctological complaints. The main results highlighted are: (i) LARs are very frequent in Congolese PLWH with proctological complaints; (ii) PLWH with LARs had a better immunological status (high CD4 count) than those who did not; (iii) hemorrhoidal disease is the most documented LAR (60.8%); and (iv) neoplastic LARs were found on histopathological examination of biopsies taken from two patients.
Our study reported a high frequency of LAR of 71.4%, highlighting the fact that the series of patients examined were more likely to be carriers of LAR due to the presence of proctological symptoms. In the United States of America, a study conducted among a group of subjects at risk of LAR, namely, men who have sex with men, reported a prevalence of LAR of 81% [19]. In contrast, several studies involving selected PLWH without reference to the presence of proctological symptoms have reported significantly lower frequencies of LAR than ours. This is particularly the case of the study by Luma et al. [20] which reported a frequency of LAR of 22.8% among PLWH in Douala, Cameroon. In the Central African Republic, however, Yassibanda et al. [21] documented a relatively high frequency of LAR in PLWH of 49.4%, suggesting that LAR remains very common even in the general PLWH population.
The observation in our study of a high frequency of LAR in a group of PLWH of whom 87.5% are treated with ARVs corroborates the conclusions of Gonzalez-Ruiz et al. [16] who did not observe an impact of the introduction of ARV triple therapy on the reduction of the incidence of LAR in PLWH. In addition to ARV treatment, we also noted that PLWH with LARs had significantly higher CD4 levels compared to those who did not have LARs, suggesting that the extent of immunodeficiency would not be a main factor influencing the appearance of LARs in these patients. This result is in line with that reported by Atipo et al. [22] in Congo-Brazzaville who reported a higher frequency of non-specific proctitis (more frequent histological lesion of the rectal mucosa in their study) in HIV-positive patients with CD4 >200 cells/mm3 compared to severely immunocompromised patients who had CD4 < 200 cells/mm3.
Our results showed that anal swelling (57.7%) and anal pruritus (35.1%) were the most reported proctological symptoms by patients. In the study by Yassibanda et al. [21] the most documented proctological complaints were proctalgia (58.6%), chronic diarrhea (53%) and anal pruritus (48.8%). In the series by Atipo et al. [22] and Fewou et al. [23] (Cameroon), anorectal pain was also the most reported anorectal symptom, respectively in 21.3% and 25.7% of PLWH, frequencies that are comparable to those observed in our study (23.8%). Constipation, hematochezia and purulent discharge were mainly found in our PVV carrying LAR, indicating the importance of a good clinical and endoscopic proctological evaluation of patients presenting these symptoms.
In terms of lesions, hemorrhoidal disease was by far the most diagnosed LAR in our PLWH (60.8%). This result corroborates the observations made in other studies on PLWH in sub-Saharan Africa [21,23]. In several other studies, on the other hand, condylomas were the most identified LAR [11,15,17,24]. In the literature, hemorrhoids, fissures (second most prevalent lesion in our series), fistulas and anal abscesses are classified as non-HIV-related diseases, whereas HIV-related LAR include proctitis (bacterial or viral), anorectal ulcerations (often of a sexually transmitted origin) and tumors (benign and malignant) [25]. In addition to the 3 confirmed cases of condyloma acuminatum, the anatomopathological examination confirmed two cases of anorectal cancer. In Brazil, the study by Nadal et al. [17] reported an incidence of anorectal cancer of 1.8% during the period 1996 and 2005, the most identified cancers being squamous cell carcinoma (59.4%) and Kaposi’s sarcoma (23.2%). These observations indicate that PLWH are at significant risk of developing digestive anorectal cancer despite ARV treatment and highlight the importance of supplementing the clinicoendoscopic evaluation of suspicious lesions with biopsy samples for histopathological analyses.
The main strength of our study is that it is one of the first studies to describe the frequency and nature of LAR in PLWH with proctological symptoms in DR Congo. As such, our study provides essential support for adapting the provision of proctological care to PLWH. However, some weaknesses are noted. First, we only included PLWH with proctological symptoms, and therefore more likely to have LAR, justifying a high frequency of LAR reported. Caution is therefore required in interpreting the results of the study, which are addressed only to PLWH with proctological symptoms and not to all PLWH. Congolese studies on LAR in the general population of PLWH are strongly encouraged. Second, histopathological analysis of LAR could only be requested in 5 patients for financial reasons. However, this limitation of the study can be put into perspective for certain LARs, such as hemorrhoidal disease (the most common LAR in our series), the diagnosis of which is essentially clinical by anoscopy [26]. Finally, our data are a little over 10 years old and could not be published due to the lack of a resource person for the analyses. Even if our data remain important on the knowledge of LARs in PLWH with proctological symptoms in the DR Congo, new studies are encouraged.
In conclusion, the present study showed that in Kinshasa, LAR are very frequent in PLWH with proctological symptoms and should be systematically sought for early diagnosis and better adapted holistic management.
Conflicts of interest: The authors declare no competing conflicts of interest.
Author’s contribution: Pauline Phaka Bikuelo: study design, data collection, patient assessment, manuscript writing, manuscript revision. Hippolyte Situakibanza Nani Tuma: study design, manuscript writing, manuscript revision. Emmanuel Bomba Di Masuangi: study design, patient assessment, manuscript revision. Tony Shindano Akilimani: study design, patient assessment, manuscript revision. Murielle Longokolo Mashi: study design, manuscript writing. Fiston Mbutiwi Ikwa Ndol: data analysis, manuscript writing, manuscript revision. Christian Kisoka Lusungi: manuscript writing, manuscript revision. Bienvenu Lebuaze Massamba: histopathological analysis of biopsy samples. Jack Kokolomami Hyombo: data analysis. Charles Mbendi Nlombi: study design, manuscript revision. Pierre Muzeke Ayol: study design. Sébastien Mbendi Nsukini: study design. Jacqueline Nkondi Nsenga: study design, patient assessment, manuscript writing, manuscript revision, study supervision.
