1Department of Pulmonary & Critical Care, Faculty of Medical Sciences, Lebanese University, Lebanon.
2Department of Internal Medicine, Faculty of Medical Sciences, Lebanese University, Lebanon.
3Pulmonary and Critical Care Division, Rassoul Aazam Hospital, Lebanon.
El Mawla Zeinab
Email: mawla.zeinab@hotmail.com
Received : Feb 19, 2025 Accepted : Mar 17, 2025 Published : Mar 24, 2025 Archived : www.meddiscoveries.org
Introduction: Subclavian vein catheterization is a common procedure for central venous access in critically ill patients. While generally safe, complications like Subcutaneous Emphysema (SE) and Pneumothorax (PTX) can arise, especially with the supraclavicular approach. These complications can be life-threatening if not promptly managed. This case highlights subcutaneous emphysema following subclavian vein catheterization.
Case presentation: An 83-year-old female with coronary artery disease, osteoporosis, and pneumonia presented with septic shock and altered mental status. During a left subclavian central venous catheter insertion for vasopressor administration, significant bilateral subcutaneous emphysema developed. Despite chest tube placement and intensive care, her condition worsened, leading to death within two days.
Discussion: The supraclavicular approach carries a higher risk of complications like subcutaneous emphysema and pneumothorax due to trauma during catheter insertion. Accidental puncture of the pleura or subclavian vessels can introduce air into the pleural space or subcutaneous tissues. Diagnosis relies on clinical signs and chest X-ray. Treatment generally involves conservative management, with more invasive measures required for severe cases. Early recognition is crucial to minimize morbidity.
Conclusion: This case illustrates the rare but significant complication of subcutaneous emphysema following subclavian vein catheterization. Despite management, the patient’s septic shock and multiorgan failure led to a poor outcome, emphasizing the importance of early detection and intervention in critically ill patients.
Keywords: Case report; Subclavian vein catheterization; Subcutaneous emphysema; Pneumothorax; Septic shock; Central venous access.
Subclavian vein catheterization is a widely utilized procedure in clinical practice for patients who require central venous access. Although it is generally regarded as a safe and effective intervention, complications can occur, particularly with the supraclavicular approach. Two notable complications are Subcutaneous Emphysema (SE) and Pneumothorax (PTX), both of which have the potential to be life-threatening if not recognized and addressed promptly [1]. Subcutaneous emphysema involves the abnormal presence of air within the subcutaneous tissues, leading to swelling and sometimes crepitus upon palpation. Pneumothorax, on the other hand, occurs when air accumulates within the pleural space, resulting in lung collapse and potentially impaired respiratory function. Early detection and management of these complications are crucial to minimize patient morbidity and ensure optimal outcomes.
Given the rarity and nonspecific pathophysiology of these complications, we will present a case to illustrate the occurrence of subcutaneous emphysema as a potential consequence of subclavian vein catheterization.
An 83-year-old female with a history of Coronary Artery Disease (CAD) status post Percutaneous Transluminal Coronary Angioplasty (PTCA) and osteoporosis with multiple vertebral fractures presented with a 2-day history of decreased consciousness, following a month-long decline in oral intake. She was a non-smoker, non-drinker, and had no known drug or food allergies. On presentation, the patient was cachectic and unresponsive, with a Glasgow Coma Scale (GCS) score of 3. Clinical examination revealed bilateral rhonchi on lung auscultation, an irregular heart rhythm (S1S2), a soft abdomen, and bilateral +3 pitting edema below the knees. Her vital signs showed hypotension (SBP 80/40 mmHg) and hypoglycemia (glucose: 32 mg/dL). An Electrocardiogram (EKG) revealed Atrial Fibrillation (AF). After dextrose administration to correct her hypoglycemia and intravenous hydration, the patient remained unresponsive and was intubated for airway protection.
Laboratory results revealed macrocytic anemia (Hb 10.6 g/dL), an elevated white blood cell count (7,800/μL, with 83% neutrophils), and thrombocytosis (408,000/μL). Inflammatory markers were significantly elevated, with C-Reactive Protein (CRP) at 29.27 mg/dL. Acute kidney injury was noted (serum creatinine 2.2 mg/dL), along with metabolic acidosis (Na 149 mEq/L, K 3.5 mEq/L, Cl 102 mEq/L, CO2 14). Mild troponin elevation (0.117 ng/mL) and hypoalbuminemia (2.2 g/dL) were also present. Urine analysis revealed white blood cells, suggesting a Urinary Tract Infection (UTI) with possible urosepsis. Imaging studies, including chest X-ray, showed right lower lobe haziness and bilateral pulmonary congestion, indicative of pneumonia. Non-contrast CT scans of the brain, chest, abdomen, and pelvis revealed chronic ischemic changes, bilateral pneumonia, and signs of chronic kidney disease.
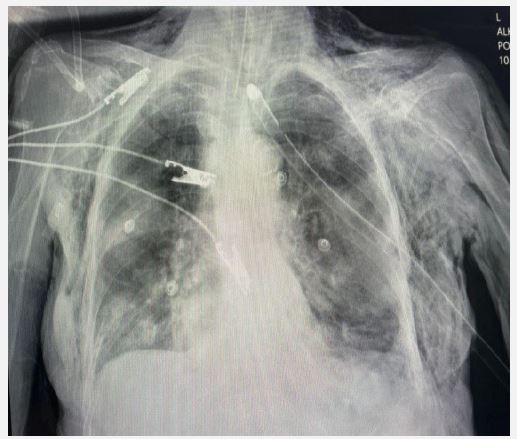
The patient was diagnosed with septic shock secondary to pneumonia and UTI. Management included broad-spectrum antibiotics, intravenous hydration, and vasopressor support for persistent hypotension. A left subclavian central venous catheter insertion for vasopressor administration was attempted but complicated by significant bilateral subcutaneous emphysema, though no pneumothorax was identified. A chest tube was inserted to manage the emphysema, with a post-procedure chest X-ray confirming appropriate placement (Figure 1). Over the next 48 hours, the subcutaneous emphysema resolved, but the patient’s hypotension persisted, and her clinical condition worsened. Despite intensive care measures, the patient succumbed to her illness after two days.
Subclavian vein catheterization, particularly via the supraclavicular approach, carries a risk of complications, including pneumothorax and subcutaneous emphysema. Although the overall incidence of these complications is relatively low, they are considered serious and potentially life-threatening [1]. Grigorakos et al. reviewed central venous catheterization complications, reporting that pneumothorax occurs in about 1.3% to 6% of cases, with a slightly higher incidence in those using the supraclavicular approach compared to other methods [2]. A systematic review and meta-analysis by Teja et al. highlighted those complications from central venous catheterization can significantly affect patient outcomes, particularly in critical care settings [3]. This underscores the importance of understanding these risks. The supraclavicular approach is favored for its anatomical advantages, but it also carries a higher risk of injuring nearby structures, including the pleura, subclavian artery, and vein. This can lead to air entering the subcutaneous tissues or pleural cavity. Subcutaneous emphysema, although less common, occurs in approximately 0.5% to 1% of subclavian catheterizations [2].
The development of subcutaneous emphysema and pneumothorax after subclavian vein catheterization is primarily due to trauma caused by the needle or catheter during insertion. In the supraclavicular approach, the subclavian vein is located near the apex of the lung and pleura. Accidental puncture of the pleura during catheter insertion may introduce air into the pleural space, resulting in pneumothorax. Additionally, air can track into the surrounding subcutaneous tissues, causing emphysema [1]. The pathophysiology of these complications involves several mechanisms: If the needle or catheter inadvertently punctures the pleura, air from the lung can enter the pleural space, causing pneumothorax. This air can then track into the subcutaneous tissues via the mediastinum. Accidental puncture of the subclavian artery or vein may also lead to air entering the bloodstream, which can spread to the subcutaneous tissues or directly enter the pleural space [2]. Subcutaneous emphysema can also occur due to barotrauma. Increased pressure from mechanical ventilation or positive pressure ventilation can force air into soft tissues, exacerbating emphysema. In severe cases, the air may spread to adjacent regions such as the neck, face, or chest wall [5].
The clinical diagnosis of subcutaneous emphysema and pneumothorax is based on the patient’s symptoms, which may include swelling, crepitus upon palpation, and respiratory distress. A hallmark sign is palpable crepitus in the neck, chest, or face due to air in the subcutaneous tissues. Radiologic imaging plays a crucial role in confirming the diagnosis and assessing the extent of the complications. A chest X-ray is typically the first imaging modality, revealing subcutaneous air, pneumothorax, or even pneumomediastinum. In some cases, a Computed Tomography (CT) scan may be necessary for a more detailed assessment of air distribution and to identify associated complications such as large pneumothorax or extensive air in the mediastinal or pleural spaces [1].
Management of subcutaneous emphysema and pneumothorax usually involves supportive care, with the approach depending on the severity of the condition. For most cases, especially when emphysema is confined to the subcutaneous tissues and the pneumothorax is small, conservative management is sufficient. Monitoring for signs of progression, such as increased respiratory distress, is essential. Chou et al. [1] report that subcutaneous emphysema typically resolves spontaneously as the body gradually reabsorbs the air. Providing supplemental oxygen can expedite the reabsorption of air from the tissues. High concentrations of oxygen increase the partial pressure gradient, helping to facilitate the diffusion of nitrogen and oxygen out of the subcutaneous tissues [4]. This therapy can also prevent the spread of air into the pleura or mediastinum. If the pneumothorax is large or causing significant respiratory distress, chest tube insertion may be necessary to evacuate air from the pleural space and relieve pressure on the lungs. Pneumothorax resulting from direct pleural puncture during catheter insertion may require chest tube placement if it causes respiratory compromise [2]. In rare cases, where emphysema is extensive or persistent, surgical intervention may be needed. This is typically reserved for situations involving severe tissue damage, persistent pneumothorax, pneumomediastinum, or infection [4].
The prognosis for subcutaneous emphysema and pneumothorax following subclavian vein catheterization is generally favorable with appropriate treatment. Most cases of subcutaneous emphysema resolve spontaneously within a few days to weeks. Similarly, patients with mild pneumothorax typically recover with minimal intervention. However, severe cases, particularly those involving large pneumothorax or mediastinal involvement, may result in prolonged hospital stays and require more invasive treatments [3]. Early recognition and intervention are crucial for improving patient outcomes and minimizing the risk of further complications.
This case illustrates the rare but significant complication of subcutaneous emphysema following subclavian vein catheterization. Despite prompt management of the emphysema, the patient’s ongoing septic shock and multiorgan failure led to a poor outcome, emphasizing the challenges in managing critically ill patients with multiple comorbidities. Early detection and intervention for complications like subcutaneous emphysema are essential to prevent further deterioration. This case reinforces the importance of careful procedural technique, vigilant monitoring, and a comprehensive treatment approach to improve patient outcomes in high-risk settings.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review upon request by the Editor-in-Chief of this journal..
Ethics approval and consent to participate: Ethical approval was not applicable.
Conflict of interest: The authors declare that they have no conflict of interest.
Financial disclosure: The authors declared that this study has received no financial support.
