1Ahmed Benbella 1 University, Oran, Algeria.
2Djillali Liabes University, Sidi Bel Abbes, Algeria.
Amel Zemmour
Email: zeam00@yahoo.fr
Received : Apr 14, 2025 Accepted : May 02, 2025 Published : May 09, 2025 Archived : www.meddiscoveries.org
Cancer-Related Fatigue (CRF) is a common and underestimated health concern among oncology patients under treatment or cancer survivors, in average 80% of patients experience CRF, it is now accepted as a diagnosis in the international classification of diseases requiring early screening and appropriate care, especially since assessment methods are available and drug and psychosocial management are effective.
Keywords: Cancer; Fatigue; Treatment.
Commonly, patients define fatigue as a distressing, persistent, subjective sense of extremely exhausted or tired, it usually occurs with pain, depression and anemia. Fatigue is a frequent symptom of cancer it can also be a complication of different specific treatments such as surgery, chemotherapy, radiation, targeted and immunotherapy or symptomatic medications.
Fatigue is underestimated in this process and only assessed by less than one third of care providers [1] it is considered as «normal» in the context of cancer and its specific therapies even in a patient with minimal or no activity, it can begin at any time: before, during or after cancer treatment.
Fatigue is experienced by 50-90% of individuals who received chemo and/or radiation, in CRF patients don’t fully recover even after sleeping or resting that’s why it should be systematically screened, assessed and managed to improve their quality of life [2-4].
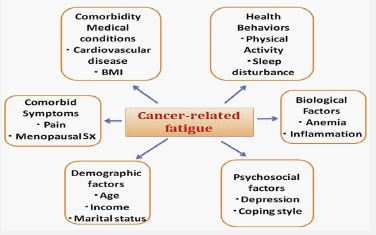
Trying to understand the mechanisms of this highly prevalent and burdensome symptom is of great interest to clinicians and researchers but unfortunately, few studies have explored the etiology of CRF, these studies have focused on factors incriminated including the disease itself, the treatments received and the physical, psychological and emotional conditions of the patient: anemia, pain, depression, anxiety, sleep disorders, biological clock disorders, immobility [5]. In addition, CRF patients exhibit greater central fatigue with a deficient drive of motor cortical output attenuating performance whereby inhibitory and excitatory processes are affected [6,7].
Causes of fatigue
A meta-analysis including 27 studies of 12.237 breast survivors showed that predictors of severe fatigue include: higher disease stage, chemotherapy treatment, chronic pain and female sex are associated with greater fatigue [8].
Many studies showed a correlation between IL 6 and CRP and other inflammatory markers levels and increased fatigue, however, the overall pathogenesis is not completely elucidated [9].
Inflammation and immune system: Cancer and its treatment can activate the peripheral pro-inflammatory cytokine network giving symptoms of CRF such as: pain, insomnia, bad mood, cognitive impairment collectively known as “sickness behavior” this neuroinflammation produced by the cytokine signaling in the central nervous system is a possible mechanism for persistent CRF [8,9].
Hypothalamic Pituitary-Adrenal (HPA) axis: Cytokines released because of cancer and/or its treatments into the CNS can stimulate the HPA axis and inhibits cortisol production, altered cortisol levels have been associated with disruption of circadian rhythm and sleep disturbance (30-75%) [10] which promotes CRF.
Reduced energy metabolism: A disrupted Adenosine Triphosphate (ATP) production after cancer treatments (chemotherapy, radiation...) can affect skeletal muscle and increase fatigue [11].
Relationship of fatigue to other symptoms
Because fatigue is a subjective condition, ill is difficult to identify some basic concepts such as [12]:
⮚ Multiple physical symptoms with affective state and the patient’s perception of illness, mood may have a crucial and long-lasting effect on eventual adaptation to chronic fatigue.
⮚ Pain and biological clock disturbance.
⮚ Depression and anxious behaviour such as restlessness and reassurance –seeking, apprehension, worry and poor concentration.
Non acceptance of cancer diagnosis and automatically specific treatments.
Given the prevalence of CRF and its impact on patient’s outcome, it is essential for clinicians and researchers not only to manage cancer patients including evaluation of prognosis but also to identify suitable treatments [13].
Screening for fatigue should include screening for possible contributing factors (pain, emotional distress, sleep disruption, anemia, and nutrition) as well as comorbid conditions (infection, cardiac dysfunction). Thus, a comprehensive assessment is required for the development of effective treatments [14] fatigue might be rated as mild, moderate or severe.
The FAS is a self-report measure requiring approximately 2 min, the following 10 statements refer to how you usually feel, for each statement you can choose one out of five answer categories, varying from never to always [15].
| Never | Sometimes | Regularly | Often | Always | |
|---|---|---|---|---|---|
| 1. I am bothered by fatigue | 1 | 2 | 3 | 4 | 5 |
| 2. I get tiredvery quickly | 1 | 2 | 3 | 4 | 5 |
| 3. I don’t do much duringthe day | 1 | 2 | 3 | 4 | 5 |
| 4. I have enoughenergy for everyday life | 1 | 2 | 3 | 4 | 5 |
| 5. Physically, I feel exhausted | 1 | 2 | 3 | 4 | 5 |
| 6. I have problems starting things | 1 | 2 | 3 | 4 | 5 |
| 7. I have problems thinking clearly | 1 | 2 | 3 | 4 | 5 |
| 8. I feel no desire to do anything | 1 | 2 | 3 | 4 | 5 |
| 9. Mentally, I feel exhausted | 1 | 2 | 3 | 4 | 5 |
| 10. WhenI am doing something, I can concentrate quite well | 1 | 2 | 3 | 4 | 5 |
However, patients with similar intensity may have widely divergent levels of disability, the visual analogic scale of fatigue is a very easy mean that score le fatigue level from 0 to 10 (extreme fatigue) [16].

Surgery: Fatigue is common after major surgery and delays recovery, this may be related to such factors as anesthesia medications, type of analgesia, decreased ventilatory capacity, immobilization, infection, anxiety. The preoperative level of depression and fatigue can also predict the prevalence of postoperative fatigue.
Chemotherapy: All chemotherapy related toxicities (nausea, vomiting, diarrhea, mucitis) can induce fatigue by reducing the food intake or causing a bothersome pain (taxanes..) other hematological side-effects such as anemia alterates tissue oxygenation, increases cardiac load and risk of fatigue under treatment and after cancer chemotherapy [5,17].
Radiation: Treatment with radiation can lead to anemia, diarrhea, weight loss, anorexia and chronic pain which can influence fatigue severity, also concurrent treatment (chemo or hormone therapy) is a known risk for persistent fatigue, radiotherapy deteriorate sleep quality, increase anxiety, anemia, cytokine activation, psychological stress, efforts to manage fatigue should focus on correcting potential etiologies and relieving symptoms [5,12,18].
Hormonal treatment: Endocrine therapy in hormone sensitive tumors such as breast, prostate and less frequently endometrial cancers especially when it is given after chemotherapy is associated with greater increases in fatigue [5,19].
Targeted therapy: VEGFR-TKIs and other molecular targeted drugs, compared to cytotoxic chemotherapies, these drugs are particularly associated with persistent fatigue, often making it difficult to continue treatment and thus disadvantaging the patient [20].
Immunotherapy: Data from prospective research on fatigue in patients receiving immunotherapy are lacking, understanding the specific mechanisms that cause immunotherapy-related fatigue is vital to develop strategies to mitigate it, recently, gut microbiome and cytokines changes have been associated with fatigue, anyway, any way in alleviating check-point inhibitors related fatigue will have a tremendous impact on the Qol of countless patients with cancer [21].
Symptomatic treatment: Polypharmacy such as central antiemetics, antihistamines, antidepressants, even some herbals and vitamins, supplements and medications, beta blockers effects and side-effects/interactions may contribute to increase bradycardia, drowsiness and fatigue [22].
After treatment: Cancer survivors report that fatigue is a disruptive symptom month or even years after treatment ends; it may affect relationships, emotions, work. Persistent fatigue deteriorate quality of life as patients become weak, too tired, heavy, slow, empty of energy to participate in the simple daily activities that make life beautiful and meaningful [23-25]; every patient feel this fatigue differently, it depends on age, type and stage of cancer, treatments received but it also depends on everyone’s reason for living and future plans, that’s why each person must find good reasons to continue to live humbly and why not happily, these reasons may be children, faith, work, hobbies or other interests…
End of life: It is likely that fatigue will increase substantially as disease progresses; at end of life some research in palliative care units reported fatigue in 100% of cases, including anorexia and lack of energy and its management needs to be a major focus of care and should be initiated to relieve or diminish suffering, although, it is recognized that some causes of fatigue cannot be assuaged [26,27].
Fatigue can manifest at any stage of cancer, and its management varies depending on the specific circumstances; various strategies can be offered to patients during specific treatments, which we will attempt to summarize.
Physical exercise: The benefits of physical exercise for the management of Cancer-Related Fatigue (CRF) in individuals with solid tumors have been established for a considerable time [28]. Recent years have seen several Randomized Controlled Trials (RCTs) in cancer patient populations demonstrating the positive effects of exercise interventions on fatigue reduction during and following cancer therapy [29]. Physical exercise is considered safe and is recommended for cancer patients receiving active treatment with curative intent, as well as for lung cancer patients undergoing surgical procedures [30]. Nevertheless, the role of exercise as an intervention for fatigue in the context of advanced cancer is less well-defined [31]. There is growing evidence that moderate physical exercise such as brisk walking (5 km/h), stationary bike, balance training and home based exercise in non-cachectic patients of at least 6 weeks can attenuate systemic inflammation and improve CRF and Qol [31-33]. Systematic reviews and meta-analysis of patients with advanced cancer indicate the Qol benefits resulting from increased physical activity may vary with stage of cancer, treatment modality and the patient’s current lifestyle [34], however, physical exercise must be used with caution in patients with bone metastases, thrombocytopenia, anemia, active infection, risk of falls [35].
Pharmacological treatments: Pharmacological interventions for Cancer-Related Fatigue (CRF) have explored various agents. Psychostimulants such as caffeine, dexamphetamine, modafinil, armodafinil, and methylphenidate, the latter a central nervous system stimulant primarily used for Attention-Deficit/Hyperactivity Disorder (ADHD) that increases dopamine levels in the CNS, have shown potential in CRF management, particularly when combined with physical activity or cognitive behavioral therapy [9,36]. Short courses of corticosteroids like dexamethasone or methylprednisolone have also demonstrated positive responses in some patients. While some studies have suggested that serotonin modulators, including Selective Serotonin Reuptake Inhibitors (SSRIs), may have an effect on CRF, the overall benefit has not been found to be statistically significant [32,37]. Additionally, haemopoietic growth factors and hormones such as melatonin or testosterone have been investigated as potential therapeutic options for CRF [38].
Despite the acknowledged importance of nutrition in the overall health and well-being of cancer patients, the evidence remains insufficient to formulate definitive dietary recommendations for the treatment of Cancer-Related Fatigue (CRF) [39]. Furthermore, current data does not support the recommendation of other nutritional supplements such as co-enzyme Q10, Guarana, Ginseng Astragalus, or L-carnitine [36].
Psychosocial intervention: Such as behavioural therapy, psychotherapy, energy conservation, support groups, changing coping strategies is recommended to improve fatigue in ECPs experienced during oncological treatment, these techniques can be helpful for the patient to identify fatigue promoting activities and develop specific strategies to avoid or modify these activities. Three trials (N 5 504) identified from existing systematic reviews qualified and form the evidence base [38-40]. One trial assessing psychoeducation plus nursing support for CRF in 103 chemotherapy naïve patients found the intervention group, compared to a standard care group, reported significantly lower levels of fatigue (P<.05) [38]. Similarly, another trial assessed the effectiveness of a psychoeducational intervention in mitigating CRF among 109 women undergoing adjuvant chemotherapy for early-stage breast cancer [41]. Results indicated that, in the short term, the control group, which received general cancer education sessions, exhibited significantly greater increases in worst and average fatigue, FACT-F, and Piper fatigue severity and interference measures immediately after the intervention (P<.05). Psychoeducation is a readily available intervention in oncology settings, often integrated into pre-chemotherapy education. This presents a valuable opportunity to prepare patients for the common experience of CRF. Research indicates that tailored psychoeducational interventions can enhance patients’understanding of CRF mechanisms, coping strategies, and overall quality of life. These interventions may also empower patients, improve self-management skills, and reduce distress associated with fatigue. However, the effectiveness of psychoeducation as a standalone treatment for CRF is inconsistent, suggesting that combining it with other evidence-based therapies may yield optimal outcomes.
Cognitive behavioural therapy: or CBT consists of muscle relaxation, cognitive restructuring and coping of training coping strategies have demonstrated a significant effectiveness in alleviating various physical and mental complications including stress and fatigue associated with cancer, further randomized clinical trials are ongoing to provide additional insights [42,43].
Yoga: Most studies showed that yoga compared with placebo improved overall Qol, fatigue and stress/distress [44,45].
Acupuncture and electro-acupuncture: Acupuncture and electro-acupuncture sessions (25-30 mn, three times weekly for 2 weeks and weekly for 6 weeks) have been suggested as efficacious and safe treatment for CRF [46,47].
Nutritional supplementation: It is necessary to check if there are nutritional deficiencies such as iron, vitamin B12 or vitamin D and supplement them, other supplements such as L-Carnithine has improved CRF compared to corticosteroïds [9,42] the use of Q10 and Guarana is controversial [48,49] there is insufficient high-quality data to support the use of ginseng as a standard treatment option for CRF [50-53].
| Recommendation | Evidence Quality | Strength of Recommendation |
|---|---|---|
| General note. The following recommendations (strong or conditional) represent reasonable options for patients depending on clinical circumstances and in the contextof individual patient preferences. Recommended care should be accessible topatients whenever possible | ||
| 1.1. Clinicians should recommendexercise (aerobic, resistance, or a combination) to reduce the severity of fatigueduring cancer treatment. Exercise should be tailored according to the individual patient’s abilities and maybe either supervised or unsupervised | Moderate | Strong |
| Note. Benefits for fatigue haveconsistently been seen with interventions that combine aerobic and resistancetraining and resistance-only interventions. The choice of exercise modality, intensity, and duration shouldbe based on several important considerations, including patient preference, availability, accessibility, likelihood of adherence, safety, and cost | ||
| 1.2.Clinicians should recommend cognitive behavioral therapy (CBT) with or without hypnosis to reduce the severityof cancer-related fatigue in adults undergoing cancer treatment | Moderate | Strong |
| 1.3.Clinicians should recommend mindfulness-based programs to reduce the severity of cancer-related fatiguein adults undergoing cancer treatment. Mindfulness-based programs mayinclude mindfulness-based stress reduction (MBSR) | Moderate | Strong |
| 1.4.Clinicians should recommend tai chi or qigong, practiced at a low to moderate intensity, to reducethe severity ofcancer-related fatigue in adults undergoing cancer treatment | Moderate | Strong |
| 1.5.Clinicians may recommend psychoeducation to reducethe severity of cancer-related fatigue in adults undergoing cancer treatment | Moderate | Conditional |
| 1.6.Clinicians may recommend American ginseng (Panaxquinquefolius) at a dose of 2,000 mg dailya to manage symptoms of cancer-related fatigue inadults undergoing cancer treatment | Low | Conditional |
| 1.7.Clinicians should not recommend wakefulness agents, such as modafinil or armodafinil, to manage symptoms of cancer-related fatigue inadults undergoing cancer treatment | Moderate | Strong |
| 1.8.Clinicians should not recommend L-carnitine to manage symptoms of cancer-related fatiguein adults undergoing cancer treatment | Low | Conditional |
| 1.9.Clinicians should not routinely recommend psychostimulants, such as methylphenidate, to manage symptoms of cancer-related fatigue inadults undergoing cancer treatment | Moderate | Conditional |
| 1.10. Clinicians should not recommend antidepressants, such as paroxetine, to manage symptoms of cancer-relatedfatigue in adults undergoing cancer treatment | Moderate | Conditional |
| No recommendation. There isinsufficient evidence to make recommendations for or against acupressure, coenzyme Q10, guarana, brain wavevibration meditation, minocycline, music or music therapy, progressive musclerelaxation, reflexology, solution-focused therapy, or yogato reduce the severity of cancer-related fatigue in adults undergoing cancer treatment | Insufficient | No Recommendation foror against |
Note: The strength of the recommendation is defined as follows: strong: in recommendations for an intervention, the desirable effects of an intervention outweigh its undesirable effects. In recommendations against an intervention, the undesirable effects of an intervention outweigh its desirable effects. All or almost all informed people would make the recommended choice for or against an intervention. Conditional/weak: in recommendations for an intervention, the desirable effects probably outweigh the undesirable effects, but appreciable uncertainty exists. In recommendations against an intervention, the undesirable effects probably outweigh the desirable effects, but appreciable uncertainty exists. Most informed people would choose the recommended course of action, but a substantial number would not. While there is no conclusive evidence regarding the optimal administration schedule, twice-daily dosing, preferably in the morning and before noon to avoid disrupting sleep patterns, may be considered.
Traditional Chinese medicine: Randomized controlled trials which investigated the use of TCM such as Chinese medicinal herbs given in the form of injections, decoctions, capsules, granules, tablets, oral solutions, powder...have shown to be beneficial in the management and treatment of CRF [54].
Other complementary therapies: Such as muscle relaxation, music therapy, hypnosis, art therapies ans stress reduction, have shown some beneficial reducing effects on CRF [55].
CRF is the most common and crucial posttreatment concern among patients with cancer, it is often not resolved by resting, clinicians need to be aware of the potential side effects of specific and non-specific therapies they use daily, also a comprehensive cancer care is necessary in collaboration with the patient’s close relatives and other care givers to ensure consistency and complementarity in care and a better Qol for the patient.
Effective management of CRF involves an informed and supportive oncology care team that assesses fatigue levels regularly, counsels and educates patients regarding strategies for coping with fatigue.
