1Department of Kinesiology and Health Education, The University of Texas at Austin, Austin, TX, USA.
2Dell Medical School, The University of Texas at Austin, Austin, TX, USA.
Hirofumi Tanaka
Email: htanaka@austin.utexas.edu
Received : May 16, 2025 Accepted : Jun 04, 2025 Published : Jun 11, 2025 Archived : www.meddiscoveries.org
Background: Physical activity is a non-pharmacological and modifiable lifestyle factor that may help reduce cardiovascular risks in large vessel vasculitis by lowering inflammation and enhancing vascular function. However, patients with this condition often encounter substantial barriers to physical activity. This paper reviews and summarizes observational and interventional studies of regular physical activity along with the barriers to physical activity in patients with large vessel vasculitis.
Methodology: Comprehensive searches of research databases were conducted to assess the challenges in being physically active and the impact of physical activity or structured exercise programs on key functional and clinical measures.
Results: Patients with large vessel vasculitis report significant fatigue, physical rigidity and pain, limb claudication, and dizziness that would lead to physical inactivity. Traditional walking programs and combined aerobic and resistance training have been shown to reduce inflammation markers, enhance vascular function, and improve physical function.
Conclusion: Although substantial barriers remain, structured physical activity represents a clinically valuable adjunct in the management of large vessel vasculitis.
Giant Cell Arteritis (GCA) and Takayasu Arteritis (TAK) are two types of large vessel vasculitis, characterized by immune-mediated systemic and vascular inflammation predominantly affecting the aorta and its major branches, leading to maladaptive vascular remodeling [1]. Patients with large vessel vasculitis are at a markedly elevated risk of severe cardiovascular complications such as aortic aneurysm, arterial stenosis or occlusion, and dissection [1], all of which contribute substantially to morbidity and mortality [2]. Although GCA and TAK share similar mechanisms that accelerate atherosclerosis and exacerbate cardiovascular complications [3-5], they affect distinct patient demographics. While TAK predominantly affects young Asian women [6], GCA preferentially affects elderly adults of Northern European heritage [7]. Both conditions are considered rare with global incidence rates ranging from 0.4 to 44 cases per 100,000 people for GCA, and up to 3.4 cases per one million individuals annually for TAK [1]. Currently, glucocorticoids in combination with a disease-modifying medication or biologic agent are considered the standard pharmacological treatment. However, glucocorticoids increase susceptibility to infections and cause adverse events [4], leading to adverse effects including muscle weakness, fatigue, and physical inactivity [8].
Regular physical activity has well-documented benefits in various chronic inflammatory diseases and has a promising role in improving complications in vasculitis diseases [7]. However, the role of regular exercise remains underexplored in large vessel vasculitis. Considering the unique vascular involvement and potential risks associated with exertion-induced vascular stress, there are uncertainties regarding the safety and appropriateness of exercise training for patients with large vessel vasculitis. Therefore, the present review aims to evaluate current evidence on the barriers affecting participation in regular physical activity and the effectiveness of physical activity interventions on cardiovascular health, physical function, and quality of life in individuals with GCA and TAK.
This review was conducted following Cochrane guidelines of reviews [9]. This was a scoping review focused on challenges and therapeutic potential of physical activity in large vessel vasculitis rather than a systematic review, therefore, it did not fit the current criteria to register with PROSPERO [10]. The findings of this research were reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines [11].
Search strategy
To address this aim, a comprehensive search strategy was applied in Web of Science, PubMed (MEDLINE) and EMBASE databases up to November 2024. To ensure the inclusion of recent and relevant data, search filters were applied to prioritize studies published within the last ten years. To enhance its specificity, medical subject headings derived from PubMed were carefully paired with additional keywords relevant to the topic. References were also searched to identify additional relevant publications. The search strategy was as below: ((Physical Activity) OR (Exercise) OR (Strength training) OR (Cardiovascular fitness) OR (Resistance training) OR (Physical fitness) OR (Physical exertion) OR (Motor activity) OR (Workout) OR (Exercise therapy) OR (Physical conditioning) OR (Physical training) OR (Recreational activities) OR (Sport activities) OR (Exercise physiology) OR (Health-related fitness) OR (Body movement) OR (Exercise intervention) OR (Ambulation) OR (Walking) OR (Steps) OR (Fatigue)) AND ((Giant Cell Arteritis) OR (Giant Cell Arteritides) OR (Horton Disease) OR (Horton‘s Disease) OR (Hortons Disease) OR (Horton’s Giant Cell Arteritis) OR (Giant Cell Aortitides) OR (Giant Cell Aortic Arteritis) OR (Giant Cell Aortitis) OR (Juvenile Temporal Arteritis) OR (Juvenile Temporal Arteritides) OR (Cranial Arteritis) OR (Cranial Arteritides) OR (Temporal Arteritis) OR (Temporal Arteritides) OR (GCA) (Takayasu Arteritis) OR (Pulseless Disease) OR (Takayasu Disease) OR (Takayasu Syndrome) OR (Takayasu’s Arteritis) OR (Takayasus Arteritis) OR (Young Female Arteritis) OR (Young Female Arteritides) OR (Aortitis Syndrome) OR (Arteritis) OR (Arteritides) OR (TAK)).
Eligibility criteria and selection
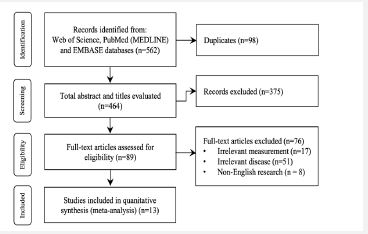
Studies were included if they involved patients diagnosed with GCA or TAK, assessing the impact of physical activity or structured exercise programs on functional, cardiovascular, or hemodynamic variables, inflammatory markers, quality of life, or pain. Studies were excluded if they focused on diseases other than GCA or TAK or lacked details about the physical activity or exercise interventions. Records were managed using Rayyan platform and Endnote software. Titles and abstracts were first screened. Full texts of selected records were assessed based on the eligibility criteria. The screening process was shown in Figure 1.
Data extraction and synthesis
Relevant data were extracted into a structured form including the first authors, years, study designs, sample characteristics (patient conditions), intervention descriptions (exercise protocols), and key outcomes/findings.
Studies related to barriers in physical activity in large vessel vasculitis
As shown in Table 1, fatigue, muscle weakness, dizziness, and claudication pain are common complaints among patients with large vessel vasculitis. Limb claudication [12] and dizziness [13,14] caused from cervical artery stenosis would lead to physical inactivity in patients with large vessel vasculitis. Additionally, patients with GCA report significant fatigue, physical rigidity (feeling stiff) and pain stemming from their disease activity or from glucocorticoid-related side effects [15,16]. Taken together, these symptoms can reduce exercise capacity/tolerance and limit the ability to engage in moderate or vigorous physical activity. Accordingly, prolonged inactivity and persistent fatigue are some of the biggest challenges of implementing or practicing regular physical activity in patients with large vessel vasculitis.
with large vessel vasculitis. Limb claudication [12] and dizziness [13,14] caused from cervical artery stenosis would lead to physical inactivity in patients with large vessel vasculitis. Additionally, patients with GCA report significant fatigue, physical rigidity (feeling stiff) and pain stemming from their disease activity or from glucocorticoid-related side effects [15,16]. Taken together, these symptoms can reduce exercise capacity/tolerance and limit the ability to engage in moderate or vigorous physical activity. Accordingly, prolonged inactivity and persistent fatigue are some of the biggest challenges of implementing or practicing regular physical activity in patients with large vessel vasculitis.
Patients with large vessel vasculitis face substantial psychological challenges, including fear of falls, loss of confidence, and a lack of motivation [15,23,24]. Negative perceptions about physical activity, such as fears of exacerbating symptoms or concerns about disease progression, may further discourage engagement in exercise programs. Indeed, patients with and without childhood-onset TAK report high levels of sedentary behavior, reduced step counts, and low engagement in moderate-to-vigorous physical activity [20,18]. Similarly, low physical activity levels and prolonged sedentary behavior have also been observed in patients with GCA [25-27]. In one survey, only 22% of GCA patients met national guidance on total physical activity [16]. Additionally, vision loss as a complication of GCA can significantly hinder the ability to engage in exercise [28].
Relevant exercise intervention studies in large vessel vasculitis
The exercise interventions in patients with large vessel vasculitis are summarized in Table 2. Because the number of available studies is very limited, a meta-analysis was not conducted in the present systematic review.
Structured exercise programs can lead to decreased inflammation and disease activity as evidenced by lower CRP and ESR [29,30]. Additionally, regular exercise may improve endothelial function by upregulating endothelial nitric oxide synthase protein expression [31].
In a case study, a GCA patient (a 71-year-old woman) participated in a three-stage exercise program lasting 40 weeks [32]. The initial three-week low-intensity walking exercise improved radial pressure, hand temperature, arm endurance, and forearm muscle oxygenation. In the second stage, progressive walking and arm pedaling were conducted for an additional 29 weeks. The functional and hemodynamic changes were further improved by continuing participation. In the last stage, resistance training for 8 weeks elicited significant improvements in upper-body muscle strength. While this study shows the feasibility and potential benefits of exercise in GCA, the nature of a case study severely limits the generalizability of the findings. To the best of our knowledge, no other exercise intervention studies exist in patients with GCA. Clearly, future research is needed to explore the potential benefits of regular exercise in patients with GCA.
In TAK, most training studies were conducted in younger populations, ranging from adolescents [33] to middle-aged adults [29]. The exercise interventions for patients with TAK show a broader diversity in exercise modes, including aerobic (endurance) exercise, resistance (strength) training, and combined multimodal programs consistently lasting for 12 weeks. The largest exercise training study to date used resistance training with corticosteroid therapy in 342 patients with TAK and produced significant reductions in inflammatory markers, including CRP, ESR, and tumor necrosis factor-α, along with reduced disease activity scores [29]. Similarly, a home-based exercise program consisted of a combination of aerobic and resistance exercise led to reductions in interleukin-1-β levels and MRI-confirmed arterial inflammation in the aorta and subclavian artery [34]. Importantly, intrahospital-supervised progressive programs using aerobic exercise training demonstrated similar benefits, such as increased levels of vascular endothelial growth factor and platelet-derived growth factor-AA alongside functional improvements in upper and lower body muscle strength [35]. These findings underscore the adaptability of exercise protocols to various settings and intensities, offering insights into program scalability and accessibility in patients with TAK. Furthermore, combining aerobic walking and resistance training showed significant improvements in walking performance metrics, such as pain-free walking distance, maximal walking distance, and six-minute walking distance along with enhanced physical functionality [36]. Interestingly, the reduction in post-exercise pain scores highlights the potential to alleviate symptoms of vascular ischemia in patients with TAK [36].
| Study | Year | Type | Participants | Physical activity challenges | |
|---|---|---|---|---|---|
| Sample (n) | Age (year) | ||||
| Austin et al. [15] | 2022 | GCA | 36 | 74 | ↑ physical symptoms (fatigue; musculoskeletal pain, aching, stiffness; glucocorticoid-related symptoms);↓ personal incapability (loss of balance, motivation and apathy; fear offalls; lack of confidence); ↑negative consequences of participating in or maintaining physical activity (difficulty building up ormaintaining fitness; new physical symptoms) |
| De Boysson et al. [17] | 2021 | GCA | 90 | 75 (60-94) | ↓ musclemass; ↑walking impairment; ↓ ability to perform dailyactivities |
| Robson et al. [16] | 2015 | GCA | 51 | 74 ± 7 | ↑ fatigue; ↑ pain; ↑ muscle weakness; ↑ physical stiffness; ↑ concerns aboutsafety |
| Dos Santoset al. [18] | 2022 | TAK | 153 | 43 (39-51) | ↓ qualityof life; ↓ physical activity; ↑ fatigue; ↓ ability to perform dailyactivities |
| Dos Santoset al. [19] | 2021 | TAK | 36 | 42 (38-46) | ↓aerobic capacity; ↓ leg-press strength; ↓ ability to perform dailyactivities; ↓ physical function; ↓ walking distance, speed and ability to climb stairs; ↓ physical activity; quality of life: ↓ general health |
| Dos Santoset al. [20] | 2021 | TAK | 72 | 42 (36-52) | ↓ gripstrength; ↓ ability to perform dailyactivities |
| Astley et al. [21] | 2021 | TAK | 34 | 18 ± 3 | ↑ sedentary time; ↓ moderate-to-vigorous physical activity; ↓ stepcounts; ↓ quality of life |
Ages are means ± SD or median (interquartile range) when applicable.
| Study | Year | Type | Participants | PA intervention | Effects | |
|---|---|---|---|---|---|---|
| Exercise/ controls (n) | Age (year) | |||||
| Manfredini et al. [32] | 2023 | GCA | 1/0 | 71 | Progressive walking and arm pedaling exercise: 2 walking/ day for 3 weeks; 2 walking and hand biking/day for 29 weeks; shoulder abduction and elbowflexion 5 reps × 4 sets for 8 weeks | ↑ radial pressure; ↑ hand temperature; ↑ arm endurance; ↑ forearm muscle oxygenation |
| Astley et al. [33] | 2021 | TAK | 5/9 | 17± 4 | Progressive aerobic mobility and bodyweight exercise training for upper & lowerlimbs and core: 1-2 sets, 3 sessions/weekfor 12 weeks | ↓ visceral fat;↓ timed up & go; ↑ timedstands repetitions; ↑quality of life;↓ arterial inflammation |
| Li et al. [30] | 2020 | TAK | 140/138 | 37± 8 | Progressive resistance training: 1 h/day,2 days/week for 12 week | ↓ ESR; ↓CRP; ↓ TNF-α; ↓ BVAS |
| Astley et al. [34] | 2019 | TAK | 12/5 | 17± 4 | Home-based resistance training: 3-4 setsof 8-12 RM, 3 days/week for 12 weeks | ↓ IL1-β;↓ MRI-confirmed arterial inflammation |
| Lanzi et al. [35] | 2018 | TAK | 1/0 | 28 | Resistance training andwalking: 30-55 min/day, 3 days/ week for 12 weeks | ↑ pain-free and maximal walking distance; ↑ timedstands repetitions; ↑ 4MVT; ↓ 5CST; ↓ stair climbing |
| Oliveira et al. [36] | 2017 | TAK | 11/10 | 35± 7 | Progressive walking program: 40-60 min/day, 2 days/week for 12 weeks | ↑VEGF; ↑ PDGF; ↑ arm curl repetitions; ↑ timed standsrepetitions; ↓ TUG;↑ stair-climbing test |
Exercise intervention in patients with large vessel vasculitis, including Giant Cell Arteritis (GCA) and Takayasu Arteritis (TAK).
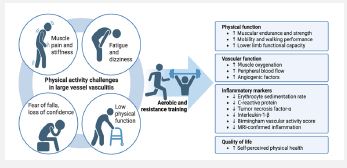
As shown in Figure 2, based on the available evidence, aerobic exercise and resistance training could be seen as feasible and effective types of physical activity for patients with large vessel vasculitis. Walking strategies, ranging from low-intensity walking to structured exercise programs, can be utilized due to their high accessibility and simplicity [36,32,35]. Walking is also a low-impact exercise with less stress on joints. The integration of resistance training is pivotal, as it directly targets muscle mass and strength, which could be compromised due to prolonged disease activity and steroid therapy [37]. The positive outcomes suggest that physical activity could promote physical health, quality of life, and psychological well-being. Exercise is well-proven to stimulate the release of endorphins to trigger a light mood and to act as a pain reliever [38]. Physical activity protocol could help alleviate depression and anxiety, which are commonly experienced by patients who bear chronic symptoms and stressors that come with large vessel vasculitis [39]. Furthermore, in a recent study [40] with primary systemic vasculitis patients, the use of wearable devices was associated with better fatigue scores and quality of life. Possibly, the use of such devices could improve lifestyle habits among patients with large vessel vasculitis. Future studies to address this are needed to provide clinical evidence. Supervised and home-based options should be provided to accommodate patient needs.
Several limitations should be noted. The rarity of large vessel vasculitis (GCA and TAK) significantly limits the availability of high quality, large-scale intervention studies. Most of the existing evidence is based on small-sample sizes, which limits generalizability and increases the potential for bias. In particular, GCA is severely underrepresented in the literature on physical activity interventions. There is a notable lack of long-term follow-up studies, making it difficult to determine the sustainability and clinical relevance of physical activity interventions over time. Future studies are needed to provide research evidence that patients with large vessel vasculitis can gain benefits from regular physical activity, addressing not only the mitigation of physical symptoms but also the enhancement of mental and emotional health and, thereby, quality of life. Practically, external facilitators, such as motivation from healthcare professionals, and personal facilitators, such as self-motivation to improve symptoms and avoid deterioration in health, should be addressed [15]. Additionally, it is noted that rheumatologists do not fully consider and provide exercise advice to patients with large vessel vasculitis [16]. Further clinical research evidence is needed to draw greater attention to the utility of exercise for these patients. To do so, more research is needed in this area.
Regular physical activity shows promise in improving cardiovascular health, physical function, and quality of life in patients with large vessel vasculitis, including GCA and TAK. However, current evidence is limited in scope, primarily short-term, and lacks standardization. Future research should focus on identifying the optimal exercise type, intensity, and duration for different patient populations and disease stages; evaluating the long-term effects of physical activity on vascular remodeling and disease progression; and developing effective strategies to enhance patient adherence. To the best of our knowledge, this is the first review focusing on physical activity interventions in large vessel vasculitis.
Funding: The authors received no funding for this work.
Competing interests: The authors declare that they have no competing interests.
Author contributions: Conceptualization: Hirofumi Tanaka, Yanbing Zhou. Writing- original draft: Yanbing Zhou, Tianyu Wang. Writing- review & editing: Curry L. Koening. Supervision: Hirofumi Tanaka
Data availability: The following information was supplied regarding data availability: This is a systematic review/meta-analysis.
