1Senior Resident, Department of Neurosurgery, Mahatma Gandhi University of Sciences and Technology, India.
2MCH Neurosurgery, Assistant Professor, Department of Neurosurgery, Mahatma Gandhi University of Sciences and Technology, India.
3MCH Neurosurgery, Professor of Department of Neurosurgery, Mahatma Gandhi University of Sciences and Technology, India.
Anmol Singh Randhawa
Tel: 8427222899;
Email: dr.anmolrandhawa@gmail.com
Received : May 09, 2025 Accepted : Jun 12, 2025 Published : Jun 19, 2025 Archived : www.meddiscoveries.org
Subdural Hematoma (SDH) is a well-recognized complication in patients on antiplatelet therapy, particularly in the elderly or those with prior cardiovascular interventions. We report the case of a 63-year-old male with a recent history of Percutaneous Transluminal Coronary Angioplasty (PTCA) on dual antiplatelet therapy who presented with a subacute SDH. He underwent burr hole evacuation with symptomatic relief. Postoperatively, blood thinners were restarted after cardiology consultation. However, the patient developed recurrent SDH which was subsequently managed with Middle Meningeal Artery (MMA) embolization. This case highlights the role of MMA embolization in recurrent SDH and the complexity of balancing antiplatelet therapy in neurosurgical patients.
Subdural Hematomas (SDH) are commonly encountered in neurosurgical practice, particularly in elderly patients or those with coagulopathy or antithrombotic therapy. Chronic or subacute SDHs can be managed conservatively or surgically, but recurrence rates remain significant, especially when patients are on anticoagulants or antiplatelet agents [1].
Middle Meningeal Artery Embolization (MMAE) is an emerging adjunct or alternative treatment option for SDH, particularly in cases of recurrence. The decision-making process becomes complex in patients who require dual antiplatelet therapy for cardiac indications such as recent PTCA [2]. We present a case illustrating this challenge and the successful use of MMAE in a recurrent SDH case.
A 63-year-old male, Mr. Ramesh Khatnanai, presented to the emergency department of Mahatma Gandhi Hospital on March 7, 2025, with complaints of holocranial headache for 3 days, which was sudden in onset, progressive, and unrelieved by medication. He also reported slurring of speech for the past 2–3 days.
He had a recent history of PTCA on February 2, 2025, and was on dual antiplatelet therapy (Ticagrelor 90 mg BID and Unistar). On examination, he was drowsy but arousable with a Glasgow Coma Scale (GCS) of E4V5M6. Neurological examination revealed left-sided weakness with UL power of 4/5 and LL power of 3/5.
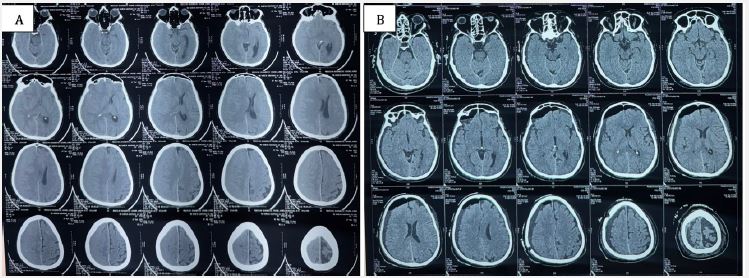
An NCCT head revealed a subacute SDH along the right fronto-parieto-temporal convexity with effacement of adjacent sulcal spaces, mass effect on the right lateral ventricle, and significant midline shift (Figure 1A). He was taken up for right-sided burr hole craniotomy and evacuation of hematoma under general anesthesia. Postoperatively, he showed marked improvement in sensorium and resolution of headache, with improvement in left-sided power to near normal.
Given his recent cardiac intervention, antiplatelet therapy was restarted postoperatively after discussion with cardiology. The patient was discharged with an intact sensorium and advised follow-up (Figure 1B).
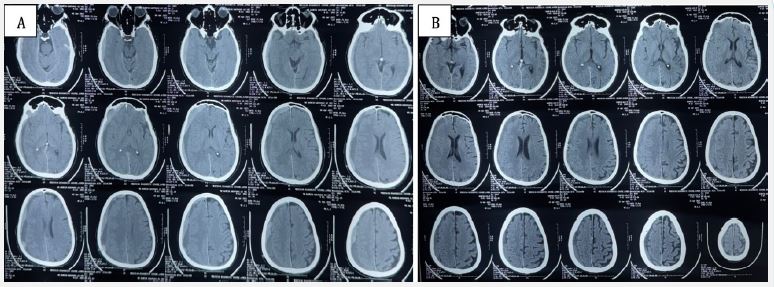
Two weeks later, the patient re-presented with acute-onset holocranial headache for 5 days, severe and non-responsive to analgesics. Repeat NCCT head showed recurrent subacute SDH with acute elements along the same right convexity (Figure 2A). There was no fresh trauma. Given the recurrence and cardiac comorbidity, he was referred to interventional neuroradiology, and underwent middle meningeal artery embolization (MMAE) on April 8, 2025.
The procedure was uneventful, and the patient remained neurologically stable postoperatively with no new deficits. On April 22, 2025, follow-up NCCT showed partial resolution of the hematoma with no fresh bleed (Figure 2B). The patient was asymptomatic and neurologically intact.
Subdural Hematoma (SDH), especially in elderly or anticoagulated patients, carries a high risk of recurrence post-surgical evacuation. Recurrence after burr hole evacuation is often attributed to the persistence of the hematoma membrane and its vascular supply via branches of the middle meningeal artery (MMA). Hence, MMA embolization has emerged as an adjunctive or alternative therapy aimed at targeting the underlying pathophysiology.
Several case series and retrospective studies have demonstrated favorable outcomes with MMA embolization. For example, Link et al. reported a 90% success rate in preventing recurrence among 60 patients treated with MMA embolization, showing it to be a minimally invasive and effective adjunctive therapy [2]. Similarly, Kan et al. reviewed 154 procedures and found significantly lower recurrence rates compared to historical surgical controls, especially in patients with comorbidities making reoperation risky [3].
Catapano et al. presented an evidence-based review supporting MMA embolization as a first-line or adjunct treatment for chronic and recurrent SDH, particularly in high-risk patients [4]. Additionally, Ng et al. emphasized the technique’s role in reducing recurrence and the need for repeat surgeries in their institutional review of 72 patients [5].
However, not all reports have been uniformly favorable. Shotar et al. (2021) reported a 22% recurrence rate post-MMA embolization in their cohort, suggesting that patient selection, technique variability, and hematoma characteristics may influence outcomes [6]. Kim (2020) noted that in cases with septated hematomas or significant acute-on-chronic components, MMA embolization alone may not suffice, necessitating surgical evacuation [7].
Therefore, while MMA embolization presents a promising minimally invasive option with a growing evidence base, it is not universally effective. The decision to opt for embolization should consider individual hematoma characteristics, clinical presentation, and patient comorbidities. In our case, the patient benefitted from MMA embolization following recurrence, underscoring its utility in carefully selected scenarios.
In this case, the dual antiplatelet therapy was an essential but complicating factor. Antiplatelet agents like ticagrelor significantly increase the risk of intracranial hemorrhage [8]. Restarting blood thinners post-craniotomy is often a dilemma, especially in patients with recent coronary stenting, as premature discontinuation can risk stent thrombosis.
MMA embolization has emerged as a promising technique to reduce recurrence in chronic or subacute SDH by interrupting the vascular supply to the outer membrane of the hematoma, which perpetuates chronic bleeding [5,9]. It has been shown to be both safe and effective, especially in high-risk surgical candidates or those with recurrence.
This case illustrates a well-coordinated interdisciplinary approach — initial surgical evacuation for symptomatic relief, careful re-initiation of antiplatelet therapy post-op, and later non-surgical intervention with MMAE upon recurrence. The patient outcome was favorable, with no neurological sequelae and imaging-confirmed resolution.
This case underscores the complexities of managing recurrent subacute SDH in patients requiring ongoing antiplatelet therapy. MMA embolization serves as an effective and minimally invasive strategy to manage recurrence, especially when balancing hemorrhagic and thrombotic risks is critical. Close multidisciplinary coordination is essential in such cases to optimize outcomes.
Patient consent: Informed written consent was obtained from the patient for publication of this case and any accompanying images. Patient identity is anonymized and confidentiality has been maintained.
