1Grigol Robakidze University, Georgia.
2Georgian National University SEU, Georgia.
3Tbilisi State University, Georgia.
4Tbilisi State Medical University, Georgia.
5Pineo Medical Ecosystem, Georgia.
Nino Chaghiashvili
Tel: +995577718964;
Email: ninochaghiashvili5@gmail.com
Received : Jun 09, 2025 Accepted : Jul 01, 2025 Published : Jul 08, 2025 Archived : www.meddiscoveries.org
Cannabis use has been associated with various short- and long-term health effects, including memory impairment, tachycardia, cognitive decline, and respiratory complications. However, literature concerning more serious conditions such as myocardial infarction and pancreatitis is still emerging.
We report a case of a 51-year-old male with a history of Coronary Artery Disease (CAD), Type 2 Diabetes Mellitus (T2DM), previous Myocardial Infarction (MI), and moderate alcohol and marijuana use. The patient presented with epigastric pain radiating to the shoulders within one hour of consuming marijuana. Laboratory results showed markedly elevated serum lipase (<35 U/L), and CT imaging confirmed acute pancreatitis. The patient was managed conservatively in an outpatient setting due to his refusal of hospitalization.
Five days later, the patient experienced new-onset chest pain following marijuana use. ECG showed ST-segment elevations in leads V2-V4, and troponin levels were elevated. Echocardiography revealed apical akinesia, and coronary angiography demonstrated thrombotic occlusion in the Left Anterior Descending (LAD) artery. A primary Percutaneous Coronary Intervention (PCI) was performed. By this point, pancreatitis had resolved, with almost normalized serum lipase levels.
This case highlights the potential cardiovascular and gastrointestinal complications associated with cannabis use.
Keywords: Cannabis; Acute pancreatitis; Myocardial infarction; STEMI; Coronary artery disease (CAD).
Cannabis, particularly Cannabidiol (CBD), has demonstrated several clinical applications, such as treating chronic pain, epilepsy, and certain neurological disorders. However, therapeutic benefits do not equate to safety, and the full spectrum of cannabis-related risks remains under investigation. This paper explores cannabis-induced conditions, such as pancreatitis and acute coronary syndrome.
Mechanism of action of cannabis
Cannabis, derived from the Cannabis sativa plant, is a widely used psychoactive substance. Its primary active compounds, Tetrahydrocannabinol (THC) and Cannabidiol (CBD), exert effects through the endocannabinoid system, interacting with CB1 and CB2 receptors. CB1 receptors, primarily located in the central nervous system, are responsible for altered perception, cognition, and mood. In contrast, CB2 receptors mediate different responses, such as anti-inflammatory processes and immune modulation [14].
CBD does not strongly bind to CB1 and CB2 receptors but activates other receptors like serotonin and TRPV1 (vanilloid receptors), producing anti-inflammatory and anxiolytic effects. Cannabis, which can be smoked, vaped, or ingested, is distributed in fatty tissues due to its lipophilic properties.
THC is metabolized by CYP450 enzymes, particularly CYP2C9, into 11-hydroxy-THC, which is more potent and contributes to psychoactive effects. 11-hydroxy-THC is further metabolized into THC-COOH, an inactive compound excreted in the urine [8].
THC induces euphoria and influences pain, anxiety, and mood by increasing dopamine release in brain reward centers. It modulates neurotransmitter systems, including glutamate and GABA, affecting pain perception and mood. CBD acts as a modulator by interacting with serotonin 5-HT1A and TRPV1 receptors, potentially reducing pain, inflammation, and anxiety without producing a “high.”
Endothelial dysfunction
Marijuana has been shown to cause endothelial dysfunction. Middlekauff, Cooper, and Strauss (2022) discussed mechanisms such as oxidative stress, elevated carboxyhemoglobin levels, and CB1 receptor activation. Increased oxidative stress in endothelial cells depletes Nitric Oxide (NO), and elevated carboxyhemoglobin levels contribute to dysfunction and accelerated atherosclerosis. CB1 receptor activation promotes vascular inflammation and endothelial dysfunction, thereby increasing cardiovascular risk [12].
Effects on coagulation
THC use has been seen to increase glycoprotein IIb/IIIa and P-selectin on membranes of platelets, and even in absence of atherosclerosis to promote acute coronary thrombosis. THC can also enhance expression of lipopolysaccharide-stimulated Tissue Factor (TF) in humans, increasing the procoagulant potential of circulating monocytes [17].
Cannabis-induced myocardial infarction
Cannabis use has been linked to various cardiovascular complications such as cardiovascular dysfunction, Deep Vein Thrombosis (DVT), Thromboembolic Complications (TEC), Pulmonary Embolism (PE), Chronic Heart Failure (CHF), Myocardial Infarction (MI), and ST-Elevation Myocardial Infarction (STEMI). It may also contribute to a hypercoagulable state, though the exact mechanisms are not fully understood.
Cannabis use can contribute to arterial stiffness, impaired diastolic function, and cardiovascular dysfunction [4], as well as myocardial infarction [16]. THC has been associated with DVT, TEC, and PE in geriatric trauma patients [2].
Cannabis, especially when used with small amounts of cocaine and alcohol, is a predisposing factor for STEMI [1]. Fontana et al. [5] reported a case in which a patient developed CHF and hypercoagulability due to major methamphetamine and cannabis co-use.
Cannabis-induced pancreatitis
The pathophysiology of cannabis-induced pancreatitis likely involves activation of pancreatic receptors CB1 and CB2, disrupting normal function, although the exact mechanism remains unknown [14].
Cases of cannabis-induced pancreatitis are rare but increasingly reported, particularly in younger individuals. Even patients without a history of tobacco or alcohol use have developed acute pancreatitis [10,13].
Using the Naranjo score to assess adverse drug reactions, a score of 6 was assigned in one study, identifying cannabis as a significant contributor after excluding other predisposing factors [6]. Retrospective and population-based studies support this association. One study found a 54% increased risk of Acute Pancreatitis (AP) in cannabis users, with an Odds Ratio (OR) of 1.56 [11]. After adjusting for key factors such as age, sex, race, smoking, and alcohol use, cannabis remained associated with a 20% increased likelihood of developing AP (adjusted OR=1.20) [15].
Associated coagulation abnormalities
Hajimoradi et al. [7] described a rare case where pancreatitis triggered a systemic inflammatory response leading to coagulation disorders due to abnormalities in the hemostatic cascade and fibrinolytic mechanisms.
A 51-year-old male with a history of CAD, T2DM, MI (four years prior), prior LAD stenting, and chronic alcohol and cannabinoid use presented with severe epigastric pain radiating to the shoulders after one hour of marijuana consumption.
The patient reported using hypoglycemic medication but could not recall the name and admitted to poor adherence.
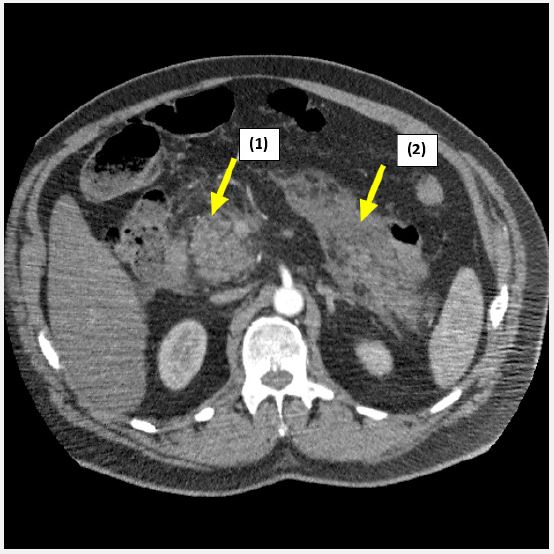
Clinical examination findings were as follows: blood pressure: 165/85 mmHg, heart rate: 90 bpm, SpO2: 97%, respiratory rate: 21. Pain relief was administered using morphine. Laboratory investigations revealed serum lipase of 331.1 U/L (normal <35 U/L). Initial ECG showed no abnormalities, and troponin levels were normal (0.037 ng/ml). CT imaging showed a mildly enlarged pancreas with peripancreatic infiltration, exudate and edema (Figure 1).
A diagnosis of acute pancreatitis was made, with no evidence of cardiac involvement. The patient was treated with Proton Pump Inhibitors (PPIs) and advised on diet and hydration in an outpatient setting due to refusal of hospitalization.
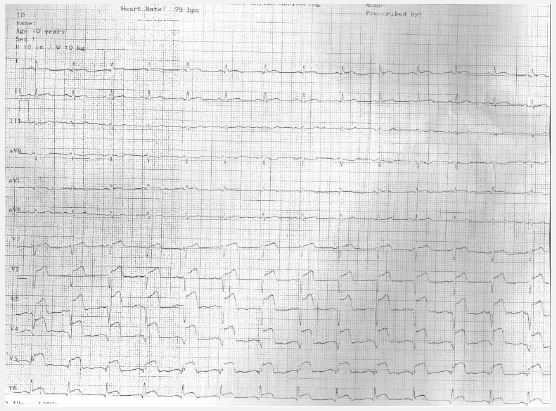
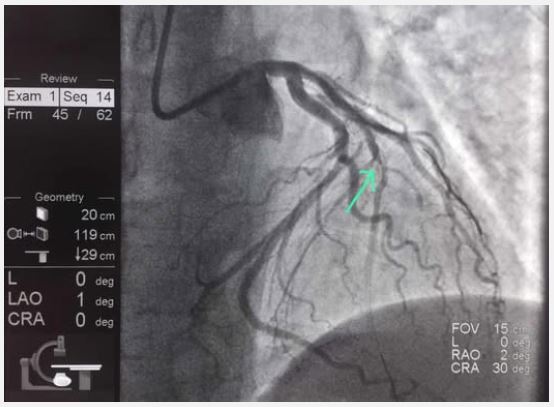
Nine days later, after consuming marijuana again, the patient presented with unstable angina. Clinical evaluation revealed normal bilateral vesicular breath sounds, a soft, painless abdomen, and no edema. Troponin level was 0.15 ng/ml (normal <0.06), ECG revealed ST-segment elevations in V2-V6 (Figure 2), and echocardiography showed apical akinesia, indicative of transmural MI. Coronary angiography revealed neoatherosclerosis with an unstable plaque and mural thrombus in the mid-segment of Left Anterior Descending (LAD) artery (Figure 3). Primary PCI was performed.
Serum lipase was reassessed and found to be almost normal (41.3 U/L. The pancreas appeared reduced in size, and pancreatitis had resolved.
This case underscores the potential cardiovascular and gastrointestinal complications of cannabis use, particularly in patients with predisposing factors and comorbidities. Cannabis use can lead to a pro-inflammatory and hypercoagulable state, contributing to both pancreatitis and myocardial infarction. While widely regarded as safe, emerging evidence suggests systemic complications associated with cannabis. Our findings align with similar cases reported by Çanga et al. [3], where a 28-year-old developed chest pain two hours after cannabis use and was diagnosed with LAD thrombosis. A case by Lawin et al. [9] described a 21-year-old who developed ST-segment elevations and LAD thrombosis shortly after cannabis consumption.
Clinicians should be aware of the potential cardiac and gastrointestinal risks associated with cannabis, even in patients with stable vitals and no significant history. Cannabis screening should be considered in cases of unexplained acute coronary syndromes and pancreatitis. Risk education is essential for patients with CAD, diabetes, or prior pancreatitis.
Given the increasing use of cannabis among young individuals, it’s crucial to educate them about its potentially serious health risks. More research is needed to establish clear pathophysiological links between cannabis use and conditions such as pancreatitis, hypercoagulability, and vascular dysfunction. Large-scale epidemiological studies are necessary to identify high-risk populations.
Conflict of interest: The authors declare no conflict or interest
Funding: This case report received no external funding.
