Medical School, St George’s University of London, Tooting, London.
El Tanani Yahia
Email: y.el-tanani@nhs.net
Received : Sep 04, 2025 Accepted : Oct 24, 2025 Published : Oct 31, 2025 Archived : www.meddiscoveries.org
Immune Checkpoint Inhibitors (ICIs) have revolutionized oncology, enabling durable remissions in cancers once deemed incurable. However, this therapeutic success is offset by Immune-Related Adverse Events (irAEs), among which the myocarditis–myositis–myasthenia gravis overlap (“Triple-M”) represents one of the most lethal complications. Despite a reported incidence below 0.3%, fulminant Triple-M carries mortality exceeding 50%, primarily due to catastrophic cardiac and neuromuscular failure. Current diagnostics—anchored in biomarkers and imaging—often fail to detect early disease, while treatment strategies remain empiric, centered on high-dose corticosteroids with variable escalation to second-line immunomodulators.
Artificial Intelligence (AI) offers a transformative opportunity. By integrating multimodal datasets—including genomics, cardiac imaging, electrocardiography, and digital health signals—AI systems can identify at-risk patients before symptom onset, enhance diagnostic precision when clinical features are nonspecific, and guide immunosuppression through adaptive algorithms that predict steroid resistance or relapse. Beyond acute care, AI-enabled monitoring via wearable devices and federated learning across global registries holds promise for reshaping survivorship and informing precision immunology.
Taken together, Triple-M overlap epitomizes both the promise and peril of immunotherapy. Harnessing precision immunology, advanced biomarkers, and AI-driven clinical intelligence is no longer optional—it is essential to transform care from reactive crisis management to proactive, predictive, and patient-centered medicine.
Keywords: Immune checkpoint inhibitors; Myocarditis; Myositis; Myasthenia gravis; Triple-M overlap; Cardio-oncology; Artificial intelligence; Biomarkers; Immunotherapy; Survivorship
Immune Checkpoint Inhibitors (ICIs) targeting PD-1, PD-L1, and CTLA-4 have transformed the management of melanoma, renal cell carcinoma, and multiple other malignancies, producing survival gains once thought unattainable [1,2]. With their expanding use, however, a parallel rise in immune-related adverse events (irAEs) has become evident, ranging from mild cutaneous reactions to fulminant multiorgan syndromes [3,4]. Among the most severe is myocarditis, which can occur in isolation or in combination with myositis and myasthenia gravis—a presentation termed “Triple-M overlap” [5-9]. Although rare, this syndrome carries strikingly high mortality, with fatalities reported even after early recognition and aggressive immunosuppression [10-13].
International registries and cardio-oncology collaborations have begun to clarify the epidemiology, clinical features, and outcomes of ICI-associated myocarditis [13,14]. Yet management remains challenged by small sample sizes, heterogeneous definitions, and reliance on retrospective analyses. Conventional tools often fail to identify high-risk patients prior to clinical deterioration, and biomarkers or imaging alone lack sufficient predictive power [19,25,26,32].
Artificial Intelligence (AI) provides a potential solution. By harnessing multimodal data—including immune signatures [24,43], advanced imaging [35-38], and global registries [14]—AI offers the ability to anticipate risk, sharpen diagnostic accuracy, and tailor therapy [16-18]. Furthermore, AI can enable adaptive trial platforms [15] and inform decision-making on rechallenge after toxicity [39,40].
Accordingly, this review aims to (i) summarize current knowledge of the epidemiology, pathophysiology, diagnostics, and management of ICI-associated Triple-M overlap; (ii) critically evaluate the challenges and gaps in evidence; and (iii) explore how emerging technologies, including Artificial Intelligence (AI), may reshape future approaches. By defining both the current state and unmet needs, this work provides a framework for clinicians and researchers navigating this rapidly evolving field.
Epidemiology and risk factors
The true incidence of Immune Checkpoint Inhibitor (ICI)–associated myocarditis remains difficult to define, with estimates ranging from 0.3% to 1.0% across clinical trials and registry data [5,6]. Rates are influenced by tumour type, therapeutic regimen, and heterogeneity in diagnostic criteria. For example, myocarditis appears more common in melanoma and renal cell carcinoma populations, where combination anti–PD-1 and anti–CTLA-4 therapy is frequently employed [1,2,7]. Within this spectrum, the myocarditis–myositis–myasthenia gravis (Triple-M) overlap has emerged as a distinct but even rarer phenotype, affecting an estimated 0.1–0.3% of ICI-treated patients [9,11]. Despite this low frequency, it is clinically significant due to its disproportionate lethality: pooled analyses and multicentre case series consistently report mortality approaching 50%, markedly higher than the 20–30% observed in isolated myocarditis [6,10-13].
Temporal clustering of events is a hallmark feature. Most cases arise early in the treatment course, with median onset between 17 and 30 days after the first ICI dose. Over three-quarters of presentations occur within the first three cycles of therapy [11,12]. This predictable time window underpins current surveillance recommendations, which emphasize vigilance during the induction phase, particularly for patients receiving dual-agent regimens.
Several clinical risk factors have been identified. Combination therapy with anti–PD-1/PD-L1 and anti–CTLA-4 agents confer the greatest risk, with rates of myocarditis several-fold higher than with monotherapy [7,8]. Patient-specific factors including older age and pre-existing autoimmune disease may contribute to vulnerability, though results are not uniform across studies [31]. Concomitant use of myotoxic drugs such as statins, colchicine, or certain antivirals has been implicated as an additional stressor on striated muscle [8].
Emerging evidence suggests genetic predisposition may shape susceptibility. Associations between HLA haplotypes (e.g., HLA-DR4, HLA-B*08) and ICI-related myositis or myastheEmerging evidence suggests genetic predisposition may shape susceptibility. Associations between HLA haplotypes (e.g., HLA-DR4, HLA-B*08) and ICI-related myositis or myasthenia gravis have been reported, highlighting the need to better understand host immune-genetic interactions [27]. As sequencing data from international registries accumulate, these associations may enable refinement of pre-treatment risk models.
Artificial intelligence offers the potential to integrate these heterogeneous risk determinants into predictive frameworks. By combining clinical variables (age, comorbidity, concomitant drugs), therapeutic details (ICI regimen, dosing schedule), and genomic features (HLA haplotypes, immune signatures), AI-driven models could stratify patients into low-, intermediate-, and high-risk categories prior to therapy [16-18,43]. Such tools could support precision oncology approaches, tailoring baseline screening intensity, biomarker surveillance, and early intervention strategies to individual patient risk.
Pathophysiology and mechanisms
The pathogenesis of ICI-associated Triple-M overlap remains incompletely understood but is likely multifactorial, involving both cellular and humoral immune dysregulation.
T-cell–mediated autoimmunity: ICIs enhance antitumor immunity by blocking PD-1/PD-L1 and CTLA-4, thereby releasing inhibitory brakes on T-cell activation [24]. While critical for tumor control, this unrestrained activity can extend to non-malignant tissues. Histopathological analyses of cardiac and skeletal muscle biopsies consistently demonstrate dense CD4+ and CD8+ T-cell infiltrates, accompanied by myocyte necrosis and macrophage activation [6-9,23].
Molecular mimicry: Autoreactive T cells may cross-react with shared striated muscle antigens, including titin and the ryanodine receptor, explaining the simultaneous involvement of myocardium and skeletal muscle (Figure 1) [27]. This mechanism aligns with the observation that myocarditis and myositis often present in parallel, with rapid clinical progression [23,28].
Humoral autoimmunity: Autoantibodies also appear contributory. Antibodies against acetylcholine receptor (AChR) and striational proteins are detected in approximately half of reported overlap cases, supporting overlap with classical myasthenia gravis [27,29,30]. Clinically, neuromuscular involvement may develop more abruptly and with greater severity than in idiopathic MG, suggesting accelerated antibody-mediated blockade at the neuromuscular junction [9,31].
Genetic and host susceptibility: Pre-existing autoimmune disease has been associated with heightened vulnerability, though causality remains debated [31]. Specific HLA alleles, including HLA-DR4 and HLA-B*08, have been preliminarily linked with risk of overlap syndromes [27], highlighting the interplay between genetic background and immune dysregulation.
AI-enabled mechanistic insights: Artificial intelligence has the potential to deepen understanding of these converging pathways. Transcriptomic profiling has already identified immune signatures predictive of myocarditis development, suggesting distinct molecular phenotypes that precede clinical toxicity [43]. Integrating genomic, transcriptomic, and immunophenotypic datasets with clinical and imaging features, AI could unravel novel pathogenic mechanisms, generate hypotheses for targeted prevention, and stratify patients by mechanistic risk profile prior to therapy initiation.
Taken together, Triple-M overlap likely arises from a convergence of unchecked T-cell activation, molecular mimicry, and autoantibody-mediated dysfunction, amplified by host geneticpredisposition. These overlapping mechanisms explain its aggressive multisystem presentation and high mortality.
Diagnostics
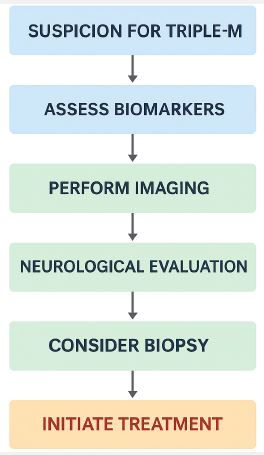
The diagnosis of ICI-associated Triple-M overlap requires early, systematic, and multimodal evaluation. Given the fulminant progression and high mortality, structured protocols that integrate clinical, laboratory, imaging, and neuromuscular assessments are essential (Figure 2 & Table 1).
Biomarkers: Cardiac troponin is elevated in over 90% of ICI myocarditis cases and remains the most sensitive marker of myocardial injury [6,21]. Serial measurement supports early detection and monitoring of treatment response. Creatine Kinase (CK) is frequently elevated tenfold above the upper limit of normal in overlap syndromes, reflecting skeletal muscle involvement [23,28]. Brain Natriuretic Peptide (BNP) and NT-proBNP may signal ventricular dysfunction but lack specificity [33]. Autoantibody testing for acetylcholine receptor (AChR), MuSK, and striational proteins is positive in approximately half of overlap cases, confirming humoral involvement and overlap with myasthenia gravis [27,29,30].
Electrocardiography and monitoring: ECG abnormalities are frequent and include atrioventricular block, sinus node dysfunction, ventricular arrhythmias, and nonspecific ST-T changes [6,8,32]. Given the risk of sudden death, continuous telemetry is recommended during hospitalization [6,10]. AI-enhanced ECG interpretation is being developed to detect subtle repolarization or conduction abnormalities, potentially enabling earlier recognition of subclinical myocarditis.
Echocardiography: Transthoracic echocardiography may show preserved ejection fraction, regional wall motion abnormalities, or systolic dysfunction. However, sensitivity is limited, as normal studies do not exclude myocarditis [6,25]. Advanced strain imaging improves detection of subclinical dysfunction and correlates with risk of adverse outcomes [21,35]. AI-driven echocardiographic analysis may further refine early detection by automating strain quantification and recognizing high-risk patterns invisible to the human eye.
Cardiac magnetic resonance (CMR): CMR, applying updated Lake Louise criteria, is the noninvasive gold standard for myocarditis, characterizing edema and late gadolinium enhancement [36]. Nevertheless, false negatives occur in biopsy-proven cases [37]. AI-based segmentation and tissue mapping may increase sensitivity by integrating subtle imaging features beyond conventional thresholds.
Positron emission tomography (PET): ^18F-FDG PET detects inflammatory uptake and is particularly useful when CMR is inconclusive. Hybrid PET-CMR approaches are being investigated to enhance diagnostic sensitivity [38]. AI-enabled image fusion and automated uptake quantification could augment reproducibility and diagnostic accuracy.
Endomyocardial biopsy: Endomyocardial biopsy remains the histopathological gold standard, revealing T-cell–predominant infiltrates with myocyte necrosis [6,8]. Its use is limited by procedural risks and sampling error. AI-supported histopathology, incorporating digital slide analysis, may improve diagnostic yield by recognizing subtle inflammatory patterns.
Neurological testing: Electromyography, repetitive nerve stimulation, and single-fiber EMG identify neuromuscular junction dysfunction consistent with myasthenia gravis [9,27,29]. Pulmonary function testing (forced vital capacity, negative inspiratory force) is crucial for anticipating respiratory compromise. AI-driven analysis of EMG waveforms could standardize interpretation and accelerate recognition of overlap syndromes.
Summary: Diagnosis of Triple-M overlap requires integration of serum biomarkers, ECG and telemetry, multimodality imaging, and neuromuscular testing. The addition of AI offers an emerging opportunity to unify disparate data streams, automate pattern recognition, and enable earlier detection before fulminant clinical deterioration.
Management strategies
Management of ICI-associated Triple-M overlap requires rapid recognition, immediate cessation of immunotherapy, and urgent initiation of immunosuppression within a multidisciplinary framework. Despite aggressive care, mortality remains high, underscoring the need for structured protocols and innovative approaches [4,19-23].
First-line therapy: High-dose intravenous corticosteroids remain the cornerstone of treatment. Intravenous methylprednisolone 500-1000 mg daily for 3-5 days is recommended, followed by a slow taper over 4-6 weeks [4]. Early initiation of steroids has been associated with improved outcomes [3,19]. Patients should be managed in monitored units with continuous telemetry, respiratory support, and access to advanced cardiac care.
Second-line and escalation therapies: For steroid-refractory cases, rapid escalation to targeted immunomodulation is advised. Abatacept, a CTLA-4–Ig fusion protein that restores T-cell tolerance, has shown efficacy in severe myocarditis and is currently under prospective evaluation in the ATRIUM trial (NCT05335928) [20]. The ACHLYS trial (NCT05716085) is investigating abatacept in combination with ruxolitinib, a Janus Kinase (JAK) inhibitor with complementary anti-inflammatory activity [6]. Mycophenolate mofetil has been successfully employed in steroid-resistant myocarditis [39]. Additional reported agents include Antithymocyte Globulin (ATG), tocilizumab, and alemtuzumab, the latter showing promise in isolated refractory cases [42]. Importantly, infliximab is contraindicated due to worsening outcomes in myocarditis [4].
Neuromuscular crisis management: Patients presenting with myasthenic crisis require prompt initiation of Intravenous Immunoglobulin (IVIG) or plasma exchange (PLEX), frequently combined with corticosteroids [41]. Early recognition of bulbar or respiratory involvement is essential, with low thresholds for ventilatory support.
Supportive measures: Supportive care may include temporary or permanent pacing for high-grade atrioventricular block, mechanical circulatory support (e.g., ECMO, Impella) in cardiogenic shock, and invasive ventilation in respiratory failure [32,33]. Optimal outcomes demand collaboration across cardiology, neurology, and critical care teams.
Emerging strategies: Novel therapies are under investigation. Alemtuzumab, targeting CD52, has shown efficacy in severe steroid- and abatacept-refractory myocarditis [42]. Adaptive immunosuppression guided by cytokine profiling represents a future direction, with machine learning models being developed to predict steroid resistance and guide early biologic initiation [19].
Artificial intelligence in triple-M overlap
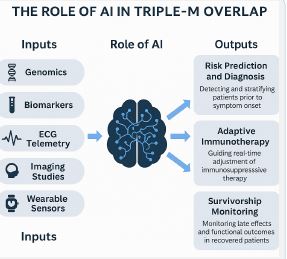
Artificial Intelligence (AI) is emerging as a transformative tool across the continuum of care for ICI-associated Triple-M overlap [16-18,43]. Unlike conventional approaches that rely on isolated biomarkers or single imaging modalities, AI has the unique capacity to integrate multimodal datasets—including genomics, serial troponins, ECG telemetry, echocardiography, Cardiac Magnetic Resonance (CMR), digital pathology, and wearable biosensor data—into unified predictive frameworks. By leveraging these diverse data streams, AI systems can generate dynamic, patient-level risk predictions, enhance diagnostic accuracy, personalize immunosuppression, and extend monitoring into survivorship.
Risk prediction and early detection
One of the most promising applications of AI lies in the early identification of patients at risk for fulminant Triple-M overlap. Machine learning models trained on registry data have demonstrated predictive capability by recognizing complex patterns in troponin kinetics, ECG telemetry, and genomic susceptibility markers such as HLA haplotypes [14,16,43]. By synthesizing these variables into composite risk scores, AI can stratify patients before symptom onset, enabling intensified monitoring during the high-risk early treatment window. Such predictive tools may ultimately shift the paradigm from reactive recognition of fulminant events to proactive prevention.
Therapeutic optimization
Beyond prediction and diagnosis, AI offers opportunities to personalize therapy. Reinforcement learning algorithms, which adapt strategies based on feedback from outcomes, may guide real-time immunosuppressive decision-making. By integrating longitudinal biomarker data, hemodynamic parameters, and clinical response, these models could predict steroid resistance and prompt earlier escalation to targeted agents such as abatacept, ruxolitinib, or mycophenolate [15,19,20,39]. Such adaptive immunomodulation has the potential to minimize treatment delays, reduce cumulative steroid exposure, and improve survival outcomes in refractory cases.
Digital health and remote monitoring
The growing adoption of wearable biosensors and mobile health platforms creates an opportunity for AI-enabled continuous monitoring beyond the hospital setting. Devices capable of tracking heart rate variability, arrhythmia burden, respirarespiratory function, and physical activity can transmit real-time data streams to predictive models [17,18]. When analysed by AI, these data may yield early warnings of disease relapse, treatment toxicity, or functional decline. This paradigm of remote, continuous monitoring could extend survivorship care into the patient’s daily life, reducing the risk of catastrophic late complications and enabling proactive intervention.
Implementation challenges
Despite its promise, the integration of AI into Triple-M overlap care faces important challenges. Concerns regarding data privacy, algorithmic bias, interpretability, and clinical workflow integration remain unresolved [18]. Federated learning approaches, which train models across multiple institutions without centralizing sensitive patient data, offer one potential solution. Moreover, robust external validation across diverse patient populations will be essential to ensure generalizability and avoid disparities in access or outcomes. Successful implementation will require not only technological innovation but also regulatory adaptation and multidisciplinary engagement across oncology, cardiology, and neurology.
Summary
AI has the potential to transform the management of Triple-M overlap by linking risk prediction, early detection, precision immunosuppression, and survivorship monitoring into a unified framework of personalized care (Figure 3). While significant barriers remain, the convergence of international registries, federated data science, and digital health integration offers a clear path forward. In the coming years, AI is likely to become an indispensable component of both research and clinical practice in cardio-oncology and neuro-oncology.
Rechallenge after triple-M
The question of whether patients who have experienced Triple-M overlap can safely undergo rechallenge with Immune Checkpoint Inhibitors (ICIs) represents one of the most contentious issues in contemporary immuno-oncology. Given the fulminant nature of this syndrome and its associated mortality, expert societies have generally recommended permanent discontinuation of ICIs in affected individuals. Nevertheless, in select oncologic contexts where therapeutic alternatives are limited, rechallenge continues to be discussed as a potential, though high-risk, strategy.
Guideline recommendations
Major societies including the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), and the National Comprehensive Cancer Network (NCCN) uniformly advise against rechallenge following severe ICI myocarditis or overlap syndromes [4,13,40]. These recommendations are based on the consistently high risk of recurrence and mortality observed in case reports and retrospective series. Unlike some other immune-related adverse events (irAEs), where rechallenge has been cautiously attempted after resolution, the catastrophic outcomes of myocarditis and overlap syndromes have led to a more conservative stance.
Clinical evidence
The available clinical evidence is limited to retrospective case series and anecdotal reports. Fatal recurrences after rechallenge have been documented, even in patients who initially appeared to have recovered fully [6,10,40]. Conversely, rare case reports describe rechallenge under intensive monitoring in individuals with mild disease or partial overlap syndromes, though outcomes remain variable [5]. Importantly, no prospective data currently support the safety of rechallenge in the context of Triple-M overlap. This profound evidence gap underscores the urgent need for systematic investigation.
Risk mitigation strategies (Investigational)
For patients in whom rechallenge is strongly considered—typically because of the absence of viable oncologic alternatives—investigators have proposed several risk-mitigation approaches. These include comprehensive baseline assessment with cardiac biomarkers, ECG, echocardiography, and neuromuscular testing prior to re-exposure [6]. Serial troponin and CK monitoring during rechallenge has been recommended to enable early detection of recurrence [7]. Advanced imaging such as weekly strain echocardiography or CMR may provide further surveillance for subclinical toxicity [8]. Ultimately, such approaches remain investigational and are feasible only within highly specialized centers, ideally under clinical trial protocols.
Oncologic alternatives
For most patients, the risk–benefit balance favors exploration of alternative strategies over ICI rechallenges. These may include targeted therapies, chemotherapy, or cellular therapies tailored to tumor type and molecular profile. Participation in clinical trials of novel immunotherapy backbones or reduced-intensity regimens may provide an additional pathway forward. Emerging AI-enabled risk stratification models may also help to define which patients, if any, could be considered for rechallenge under structured protocols in the future.
Summary
At present, rechallenge after ICI-associated Triple-M overlap is generally contraindicated due to the high risk of recurrence and death. In rare circumstances, such as in patients with limited oncologic alternatives, rechallenge may be considered only within expert centers, under strict multidisciplinary monitoring, and with full informed consent. Future research must focus on identifying predictive biomarkers and AI-enhanced surveillance strategies that could allow prospective stratification of risk, thereby clarifying whether any subgroup of patients might safely undergo re-exposure.
Future directions
Immune Checkpoint Inhibitor (ICI)–associated Triple-M overlap remains one of the most fulminant immune-related adverse events, with mortality consistently exceeding 40–50% in published cohorts [6,10-13]. Despite growing recognition and advances in acute management, progress has been limited by the rarity of this syndrome, variability in diagnostic criteria, and the lack of randomized clinical trials. Future research must therefore expand across several interconnected domains: biomarker discovery, artificial intelligence (AI)–enabled prediction and monitoring, novel therapeutic pathways, survivorship outcomes, global collaboration, and clinical trial innovation.
Biomarker discovery and risk stratification
A central priority for future work is the identification of biomarkers that can reliably predict susceptibility to Triple-M overlap. Current markers such as troponin and creatine kinase (CK) are highly sensitive for established tissue injury but lack predictive capacity. Genetic studies suggest that HLA haplotypes, including HLA-DR4 and HLA-B*08, may predispose individuals to overlap syndromes, although findings remain preliminary and require replication in larger cohorts [27,31]. High-throughput immunogenomic profiling—such as whole-exome sequencing, single-cell RNA sequencing, and T-cell receptor repertoire analysis—offers a promising avenue for uncovering genomic and immunologic determinants of risk [24,43].
Circulating biomarkers beyond troponin and CK also warrant systematic investigation. Cytokines such as interleukin-6 and tumor necrosis factor-α, along with soluble immune checkpoints, may provide dynamic signals of impending immune dysregulation. Proteomic and metabolomic profiling could reveal unique molecular signatures that distinguish Triple-M overlap from isolated myocarditis or idiopathic neuromuscular disorders. Integrating these multidimensional datasets through AI-driven models may yield composite risk scores that outperform any single marker and enable precision surveillance prior to symptom onset [16-18,43].
Artificial intelligence and digital health
AI is poised to become a transformative tool across the entire spectrum of Triple-M overlap, from prediction to survivorship. At the preclinical stage, machine learning models trained on registry data have demonstrated the ability to forecast myocarditis using longitudinal troponin trends, ECG telemetry, and genomic features [14,16,43]. These models can stratify patients by baseline risk and potentially guide decisions about the intensity of monitoring during the earliest cycles of ICI therapy.
For diagnostics, AI-enhanced interpretation of ECGs, automated strain analysis in echocardiography, and advanced CMR tissue mapping can increase sensitivity for subclinical disease, addressing the limitations of conventional imaging where false negatives remain common [17,21,35-37]. Natural language processing of electronic health records may further enhance early detection by identifying subtle documentation of symptoms such as fatigue, myalgia, or arrhythmias that clinicians might overlook [18].
In management, reinforcement learning approaches could provide real-time therapeutic optimization by predicting steroid resistance and prompting earlier escalation to agents such as abatacept, ruxolitinib, or mycophenolate [15,19,20,39]. Finally, digital health platforms and wearable biosensors capable of monitoring heart rate variability, arrhythmias, respiratory function, and activity levels can be integrated with AI to provide continuous remote monitoring, issuing automated alerts for clinicians and patients alike [17,18]. Importantly, federated learning models, which allow training across distributed international datasets without centralizing sensitive data, offer a pragmatic solution to the dual challenges of data scarcity and patient privacy (Figure 3, Table 2) [18].
Novel therapeutic pathways
Therapeutic strategies for Triple-M overlap remain dominated by corticosteroids, yet outcomes in steroid-refractory patients remain poor. Emerging targeted therapies are therefore of central interest. Abatacept, a CTLA-4–Ig fusion protein that restores T-cell tolerance, has shown encouraging results in early reports and is under prospective evaluation in the ATRIUM trial (NCT05335928) [20]. The ACHLYS trial (NCT05716085) is exploring abatacept in combination with ruxolitinib, a Janus kinase inhibitor that may suppress hyperinflammatory pathways resistant to conventional therapy (Table 2) [6].
Other immunomodulatory strategies include IL-6 blockade with tocilizumab, T-cell depletion with antithymocyte globulin or alemtuzumab, and selective B-cell depletion with rituximab [39,42]. Experimental strategies such as regulatory T-cell infusion and tolerogenic dendritic cell therapies remain at the preclinical stage but represent conceptually attractive avenues to restore immune tolerance without compromising antitumor activity. A future precision immunology framework may involve adaptive immunomodulation guided by real-time immune profiling—integrating cytokine assays, flow cytometry, and transcriptomics with AI-driven analysis to calibrate the intensity of immunosuppression in a patient-specific manner.
Survivorship and long-term outcomes
While acute mortality has understandably dominated research focus, survivors of Triple-M overlap frequently experience long-term complications. Cardiac sequelae include persistent left ventricular dysfunction, arrhythmia burden, and conduction abnormalities, while neuromuscular consequences such as proximal weakness, ocular or bulbar deficits, and chronic fatigue significantly impair quality of life [33]. The psychosocial impact of prolonged intensive care admissions and treatment interruptions adds further complexity, contributing to depression, anxiety, and diminished functional recovery.
Future research must systematically incorporate long-term follow-up and patient-reported outcomes into registries and clinical trials. Survivorship care should be organized within multidisciplinary clinics that integrate oncology, cardiology, neurology, rehabilitation, and mental health. Digital health platforms and wearable technologies, when combined with AI-driven analytics, may extend survivorship care into the home environment, allowing continuous monitoring and proactive interventions that address chronic morbidity.
Global registries and collaborative networks
Because Triple-M overlap is rare, international collaboration will be essential to generate adequately powered datasets. Expanding existing cardio-oncology registries to specifically capture overlap syndromes, with standardized definitions and harmonized data elements, represents a critical step [13,14]. The integration of biospecimen repositories into these registries would allow linkage of clinical data with translational research, accelerating biomarker discovery and mechanistic insights.
AI-enabled federated learning approaches could allow predictive models to be trained across multiple registries without compromising patient privacy, thereby enhancing both robustness and generalizability [18]. Beyond data science, collaborative networks must prioritize dissemination and clinician education, ensuring that providers across oncology, cardiology, and neurology are prepared to recognize early warning signs and deliver guideline-concordant management in real-world settings.
Clinical trial innovation
Conventional randomized controlled trials are ill-suited for rare, fulminant toxicities such as Triple-M overlap. Innovative trial designs will therefore be critical. Adaptive platform trials, which enable the simultaneous evaluation of multiple therapeutic strategies within a single infrastructure, offer a particularly efficient approach [15]. Basket trials spanning multiple immune-related toxicities could further enhance feasibility by increasing the pool of eligible patients. Embedding trial recruitment and randomization within international registries would not only streamline enrollment but also enhance generalizability.
AI integration may add further value by optimizing patient selection, refining composite endpoints, and enabling dynamic adaptation of trial arms based on interim data. Bayesian adaptive methodologies could allow early stopping for efficacy or futility, conserving resources and accelerating therapeutic discovery. Together, these innovations could overcome the limitations of small sample sizes and heterogeneity, which have historically constrained progress in this field.
Summary
The future of research and clinical care in ICI-associated Triple-M overlap lies in the convergence of biomarker discovery, AI-enabled prediction, targeted therapeutic development, survivorship care, global collaboration, and innovative trial designs. Artificial intelligence, in particular, has the potential to unify these domains, transforming fragmented data into actionable insights and guiding personalized strategies for prevention, diagnosis, therapy, and long-term monitoring. By shifting from reactive management of catastrophic presentations to proactive, predictive, and individualized care, the field can meaningfully improve outcomes in this uniquely lethal syndrome.
| Domain | Findings | Strengths | Limitations |
|---|---|---|---|
| Biomarkers | ↑ Troponin (>90%), ↑ CK (often >10× ULN), ↑ BNP/NT-proBNP (variable), Autoantibodies (AChR, striational) | High sensitivity (troponin, CK); supportive of overlap syndrome | Nonspecific; overlap with other causes of cardiac/muscle injury |
| ECG/Telemetry | AV block, ventricular arrhythmias, sinus node dysfunction, ST-T changes | Detects arrhythmias; continuous monitoring possible | Low specificity; subtle changes easily missed |
| Echocardiography | Variable LVEF; wall motion abnormalities; strain abnormalities | Widely available; non-invasive | Limited sensitivity in early disease |
| CMR | Myocardial edema; LGE (Lake Louise criteria) | Gold-standard noninvasive imaging; tissue characterization | False negatives in patchy/early disease |
| FDG-PET | Myocardial inflammatory uptake | Complementary to CMR; useful when CMR inconclusive | Limited availability; standardization lacking |
| Biopsy | CD4+/CD8+ infiltrates; myocyte necrosis | Diagnostic gold standard | Invasive; sampling error |
| Neurology testing | EMG, single-fiber EMG, respiratory muscle testing | Confirms MG overlap; ventilatory risk | Requires expertise; invasive |
| Therapy | Setting | Evidence | Limitations |
|---|---|---|---|
| High-dose corticosteroids | First-line | Improved outcomes with early initiation [3,19] | Steroid-refractory disease remains common |
| Abatacept (CTLA-4–Ig) | Steroid-refractory; under trial (ATRIUM) | Case reports + ongoing RCTs [20] | Limited data; availability |
| Ruxolitinib (JAK inhibitor) | Steroid-refractory; combined with abatacept (ACHLYS) | Preclinical + trial stage [12] | Early-phase only |
| Mycophenolate mofetil | Steroid-resistant myocarditis/overlap | Case reports [39] | Not validated in trials |
| IVIG / Plasma exchange (PLEX) | Myasthenic crisis | Established in MG [10,41] | Supportive; does not target T-cell pathogenesis |
| Alemtuzumab (anti-CD52) | Steroid/abatacept-refractory myocarditis | Anecdotal reports [42] | High toxicity; very limited evidence |
| Tocilizumab (IL-6 blockade) | Steroid-refractory myocarditis | Small case reports [39] | Insufficient data |
| Supportive measures | AV block (pacing), cardiogenic shock (ECMO/Impella), ventilatory support | Life-saving in fulminant cases | Requires advanced centers |

Immune Checkpoint Inhibitor (ICI)–associated Triple-M overlap, comprising myocarditis, myositis, and Myasthenia Gravis (MG), has emerged as one of the most severe immune-related adverse events (irAEs) in modern oncology. Although the incidence is rare (<0.3%), its lethality is disproportionately high, with fulminant cases carrying a mortality rate of 40–50% [1–2]. The present review integrates evidence across epidemiology, mechanisms, diagnosis, therapeutics, and survivorship while emphasizing the transformative potential of Artificial Intelligence (AI) and global collaboration in reshaping future care.
Epidemiology and early recognition
Epidemiologic data consistently demonstrate that Triple-M overlap arises early in the course of ICI therapy, often within the first three cycles [3,6,11]. This narrow temporal window highlights both an opportunity and a challenge: patients must be closely monitored during initial treatment, yet early symptoms are often nonspecific. Systematic incorporation of cardiac and neuromuscular biomarkers—particularly serial troponin and Creatine Kinase (CK)—into early-cycle surveillance protocols may improve detection. Structured algorithms that combine biomarker monitoring with symptom checklists, ECG telemetry, and baseline echocardiography could reduce diagnostic delays and avert catastrophic presentations.
Mechanistic insights
The pathophysiology of Triple-M overlap reflects the convergence of cellular and humoral autoimmunity. Unrestrained T-cell cytotoxicity, driven by PD-1/PD-L1 and CTLA-4 inhibition, promotes infiltration of myocardium, skeletal muscle, and neuromuscular junctions [4,5]. Molecular mimicry involving striated muscle antigens such as titin and the ryanodine receptor appears to underlie the synchronous involvement of cardiac and skeletal tissues. In parallel, humoral mechanisms—including autoantibodies against acetylcholine receptors—accelerate neuromuscular dysfunction, often producing more abrupt MG presentations than idiopathic disease. Preliminary links between specific HLA haplotypes (e.g., HLA-DR4, HLA-B*08) and susceptibility further support an immunogenomic contribution to risk [6,27,31]. These mechanistic insights not only explain the aggressive clinical phenotype but also highlight avenues for future biomarker discovery and precision risk stratification.
Diagnostic paradigms
Diagnosis of Triple-M overlap remains challenging due to its heterogeneity and the imperfect sensitivity of individual modalities. Troponin and CK elevations remain the most widely used diagnostic anchors, but their specificity is limited. Advanced imaging techniques have expanded the diagnostic toolkit: Cardiac Magnetic Resonance (CMR) using the Lake Louise criteria and FDG-PET imaging provide complementary insights into myocardial inflammation [7,8,38]. Nevertheless, CMR false negatives are not uncommon, even in biopsy-proven myocarditis [37], underscoring the importance of multimodality integration. Endomyocardial biopsy remains the gold standard but is limited by procedural risk and patchy disease distribution [36].
Neurological testing—including electromyography, repetitive nerve stimulation, and pulmonary function testing—is critical for characterizing MG overlap and anticipating ventilatory failure [10,27]. Looking ahead, AI-enabled diagnostic augmentation holds particular promise. Deep learning algorithms applied to ECGs, echocardiographic strain imaging, and CMR tissue characterization may increase sensitivity for subclinical disease, while natural language processing of electronic health records could identify early symptom constellations that escape clinical detection [17–18].
Therapeutic advances
High-dose corticosteroids remain the cornerstone of initial management, with early initiation linked to improved outcomes [3,19]. Yet outcomes in steroid-refractory cases remain poor, underscoring the urgent need for escalation strategies. Abatacept, a CTLA-4–Ig fusion protein, is the most advanced biologic therapy under investigation and may soon redefine standard of care if results from the ATRIUM trial prove positive [11,20]. The ACHLYS trial is evaluating abatacept in combination with ruxolitinib, a Janus kinase inhibitor with the potential to suppress hyperinflammatory pathways resistant to steroids [12].
Additional strategies include IL-6 blockade with tocilizumab, T-cell depletion with antithymocyte globulin or alemtuzumab, and selective B-cell depletion with rituximab [39,42]. Experimental approaches such as adaptive cytokine-guided immunomodulation and reinforcement learning–driven therapy adjustment may further refine treatment, minimizing both under- and overtreatment. AI-driven prediction of steroid resistance represents a particularly promising area, with early models suggesting potential for guiding individualized escalation strategies [15,19].
Rechallenge controversy
The question of whether patients who survive Triple-M overlap can safely be rechallenged with ICIs remains one of the most contentious issues in immuno-oncology. Major guidelines—including those of ASCO, ESMO, and NCCN—unanimously recommend permanent discontinuation following severe ICI myocarditis or overlap syndromes, reflecting the high risk of recurrence and death [13,40]. Fatal relapses after rechallenge have been reported even in patients who initially appeared to recover fully [6,10].
Although isolated case reports describe successful rechallenge under intensive surveillance in select patients with mild or incomplete overlap syndromes, these remain anecdotal and insufficient to alter current practice [5]. At present, rechallenge should only be considered in exceptional circumstances within expert centers, supported by comprehensive baseline evaluation, intensive biomarker and imaging surveillance, and fully informed patient consent. Prospective studies, potentially aided by AI-enhanced risk stratification, will be essential to determine whether any subgroup of patients might safely undergo re-exposure.
Survivorship considerations
Long-term outcomes in survivors of Triple-M overlap remain poorly defined but are increasingly recognized as clinically significant. Persistent left ventricular dysfunction, arrhythmia burden, and conduction abnormalities are common, alongside neuromuscular sequelae such as proximal weakness, ocular or bulbar deficits, and chronic fatigue [19,33]. These complications profoundly impair functional recovery and quality of life. Prolonged intensive care admissions and treatment interruptions further contribute to psychosocial distress and anxiety, underscoring the need for survivorship frameworks that extend beyond acute care.
Multidisciplinary survivorship clinics that integrate oncology, cardiology, neurology, rehabilitation, and mental health services may offer a structured approach to recovery. Incorporating patient-reported outcomes and longitudinal quality-of-life metrics into registries will also be crucial. Here too, digital health platforms and AI-enabled monitoring may extend survivorship care into the home, enabling proactive detection of late complications and facilitating personalized rehabilitation pathways.
Artificial intelligence and global collaboration
AI offers unique opportunities to unify fragmented diagnostic, therapeutic, and survivorship data into actionable clinical tools. By integrating biomarker kinetics, ECG telemetry, imaging modalities, genomic data, and wearable biosensor outputs, machine learning models can identify at-risk patients and guide adaptive immunosuppression [16-18,43]. Natural language processing can enhance early detection by extracting subtle symptom patterns from unstructured health records [18], while reinforcement learning may inform dynamic treatment strategies in steroid-refractory disease [15,19].
Global collaboration is equally vital. International registries and biospecimen repositories will provide the scale necessary to power biomarker discovery and validate AI tools [13,14]. Federated learning approaches—training AI models across institutions without centralizing patient data—may balance the need for large-scale analytics with privacy protection [18]. Finally, adaptive platform trials embedded within registries represent a promising model for evaluating novel therapies efficiently in this rare but devastating syndrome [15].
Summary
Triple-M overlap exemplifies the dual-edged nature of immune checkpoint blockade: a therapy that transforms cancer outcomes yet carries the risk of catastrophic autoimmunity. This review underscores the need for standardized diagnostic definitions, validated predictive biomarkers, and randomized evaluation of novel immunomodulators. AI and digital health tools, coupled with global collaboration and innovative trial design, provide the most promising pathway toward earlier detection, more effective treatment, and improved survivorship. By integrating these advances into clinical practice, the field may shift from reactive crisis management to proactive, precision-guided care in ICI-associated Triple-M overlap.
Limitations
This review has several important limitations. First, most available data on ICI-associated Triple-M overlap are derived from retrospective registries, pharmacovigilance databases, and case series, which limits causal inference and generalizability [5,6,10,19,32]. Prospective studies remain scarce, and reported outcomes may be influenced by selection bias and under-reporting. Second, diagnostic definitions vary considerably across studies, with inconsistent use of Cardiac Magnetic Resonance (CMR), FDG-PET, and biopsy, leading to heterogeneity in case ascertainment [36-38]. Even gold-standard modalities such as CMR demonstrate false negatives in biopsy-proven myocarditis, underscoring the challenges of standardization [37].
Third, evidence for therapeutic strategies beyond corticosteroids is limited primarily to anecdotal reports and small case series. Agents such as abatacept, ruxolitinib, and alemtuzumab are supported by early-phase trials or compassionate use reports, but robust randomized data are lacking [20,39,42]. Fourth, the role of artificial intelligence in Triple-M overlap, although conceptually transformative, is largely based on extrapolation from general oncology and cardiovascular medicine [16–18,43]. Validation in large, multicenter, and ethnically diverse cohorts is still pending, and issues of algorithmic bias and data privacy require resolution [18].
Finally, survivorship outcomes remain poorly characterized. Long-term cardiac and neuromuscular morbidity, quality of life, and cancer outcomes following ICI discontinuation are rarely captured systematically [19,33]. Existing studies are limited by short follow-up, incomplete functional assessment, and lack of patient-reported outcomes. Together, these limitations highlight the urgent need for standardized diagnostic criteria, prospective international registries, adaptive clinical trial designs, and robust AI validation to advance the field.
Immune Checkpoint Inhibitor (ICI)–associated Triple-M overlap, comprising myocarditis, myositis, and myasthenia gravis, represents one of the most fulminant and life-threatening immune-related adverse events in oncology. Although rare in incidence, its disproportionate lethality demands systematic strategies for prevention, early recognition, and precision management. Over the past decade, mechanistic insights have clarified the convergence of T-cell cytotoxicity, molecular mimicry, and autoantibody-mediated dysfunction as key drivers of this syndrome, while epidemiologic studies have consistently shown that risk is greatest within the earliest cycles of therapy.
Despite progress, major gaps remain. Diagnostic algorithms are hindered by nonspecific presentations and imperfect sensitivity of current tools. Therapeutically, corticosteroids remain the cornerstone of management, yet outcomes in steroid-refractory cases remain poor. Novel strategies under investigation—including abatacept, ruxolitinib, and cytokine-directed therapies—hold promise, but require validation through ran domized, adaptive clinical trials. Survivorship outcomes remain underexplored, with many patients experiencing persistent cardiac and neuromuscular morbidity that impairs long-term quality of life.
Artificial Intelligence (AI) provides a transformative opportunity to unify these domains. By integrating multimodal data streams—ranging from genomics and biomarkers to imaging, electrophysiology, and digital health—AI can enable predictive risk stratification, augment diagnostic accuracy, guide adaptive immunosuppression, and extend monitoring into survivorship. Federated learning approaches, trained across international registries, may overcome data scarcity while protecting patient privacy.
Moving forward, the convergence of precision immunology, AI-enabled tools, and global collaboration will be critical. Standardized diagnostic frameworks, validated biomarkers, registry-embedded platform trials, and survivorship-focused care models must collectively define the next phase of research and clinical practice. Through these innovations, the field can shift from reactive crisis management toward proactive, predictive, and patient-centered care, ultimately improving both survival and quality of life for patients affected by ICI-associated Triple-M overlap.
