1School of Pharmaceutical Sciences, Glocal University Mirzapur Pole, India.
2School of Pharmaceutical Education and Research Jamia Hamdard, India.
3Department of Research and Development, AIMIL Pharmaceuticals, India.
4Glocal University Pharmacy College, Mirzapur Pole, India.
Kiran Dubey
Email: kdubay@jamiahamdard.ac.in
Received : Oct 08, 2025 Accepted : Nov 21, 2025 Published : Nov 28, 2025 Archived : www.meddiscoveries.org
Rapid progress in vaccine development was prompted by the unprecedented global health challenge posed by the emergence of the novel coronavirus disease (COVID-19) caused by SARS-CoV-2. The current state of COVID-19 vaccines, including their technological platforms, efficacy, safety, and worldwide distribution, is summarized in this review. It discusses the outcomes of clinical trials and the practical efficacy of the main vaccine types, including mRNA-based, viral vector, protein subunit, and inactivated virus vaccines. Challenges like vaccine hesitancy, equitable distribution, and the emergence of variants of concern that could affect vaccine efficacy are also covered in the review. Lastly, it looks at potential future paths, such as ways to improve pandemic preparedness, booster shots, and next-generation vaccines. A thorough grasp of the changing COVID-19 vaccination landscape and its vital role in pandemic control is the goal of this synthesis.
Keywords: SARS-CoV-2; COVID-19; Vaccines; Safety; Efficacy; Pandemic.
Reported in December 2019 in Wuhan, the capital of Hubei province in China, the first instances of coronavirus disease 2019 (COVID-19) have been recorded to cause severe respiratory diseases including pneumonia and lung failure. The fast-increasing number of diseases spread throughout China and then over the world. Originally known to as 2019-nCoV or the Wuhan Coronavirus, the sickness COVID-19 was formally identified by the World Health Organisation (WHO). The virus responsible Close proximity of the virus to the severe acute respiratory syndrome coronavirus (SARS-CoV), which started an epidemic in 2002, was found by genetic investigations. As such, the International Committee on Taxonomy of Viruses (ICTV) assigned the virus SARS-CoV-2 [1,2].
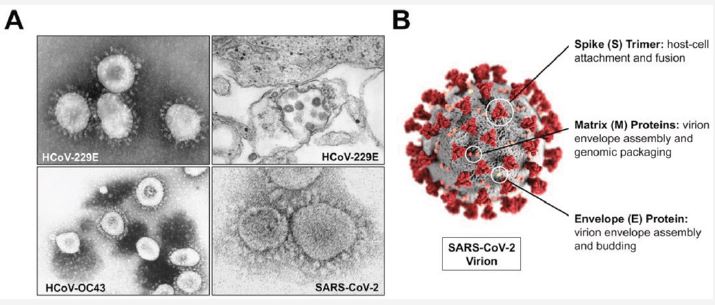
SARS-CoV-2 belongs to the Coronaviridae family, characterized by enveloped, positive-sense single-stranded RNA ((+)ssRNA) Viruses. It is believed to have arisen from zoonotic coronaviruses, including SARS-CoV, and has been recognized as the causal agent of COVID-19. Subsequent to its first identification, SARS-CoV-2 swiftly disseminated globally, resulting in a pandemic. As of April 13, 2024, there have been over 704,753,890 crores confirmed cases worldwide and more than 7,010,681 lakh deaths. India recorded approximately 45,035,393 crores cases and 533,570 fatalities, according to statistics from https://www.worldometers.info/coronavirus/#countries [3,4].
The exact origin of the SARS-CoV-2 outbreak remains unclear, but hypotheses suggest bats [5], snakes [6], or pangolins [7,8] may have acted as the virus’s vectors. COVID-19 symptoms tend to be more severe in older adults with preexisting conditions, such as asthma, Chronic Obstructive Pulmonary Disease (COPD), and other allergic diseases [9,10]. Given the severe impact of the pandemic on human lives and economies worldwide, understanding the current situation and implementing effective strategies to mitigate the virus’s spread are critical. Although various diagnostic kits for COVID-19 are available and some repurposed therapeutic agents have been tested, none have yet demonstrated significant efficacy in clinical trials [64,65].
Vaccines are a more cost-effective solution than treatment and can reduce morbidity and mortality without long-term side effects [11,12]. Preventive and therapeutic vaccines are essential to combating infectious diseases and safeguarding global health [13,14]. In the last two decades, three significant human coronaviruses—SARS-CoV, MERS-CoV, and SARS-CoV-2—have emerged, posing substantial threats to global health [15]. Research teams worldwide are accelerating COVID-19 vaccine development using various strategies. As of Dec 2, 2022, 50 vaccines were approved for limited or emergency use, while 16 vaccines had full approval [16].
Understanding the precise mechanisms of viral recognition and host interaction is vital for studying host tropism, cross-species transmission, and vaccine development. The spike (S) protein of SARS-CoV-2, which enables viral entrance by binding to host cell receptors, is a pivotal target for vaccine development. This protein interacts with many host receptors, including ACE2 (used by SARS-CoV-2 and SARS-CoV), APN, and DPP4 [17-19]. The Receptor-Binding Domain (RBD) inside the S1 subunit of the spike protein is crucial for receptor recognition, while the S2 subunit enables membrane fusion between the virus and host cells [20-22]. SARS-CoV-2 shares approximately 75% homology in the spike protein RBD with SARS-CoV [20].
Globally, more 200 vaccines are under development, with 38 Indian pharmaceutical companies contributing to these efforts. Currently, 66 vaccines are in phase 1 trials, 72 in phase 2, 93 in phase 3, and 50 have been authorized for use. As of Dec 2, 2022, more than 13.64 billion vaccine doses had been administered worldwide, with 67% of the global population fully vaccinated. In India, over 2.21 billion doses had been given, with 74% of the population fully vaccinated as 31 December 2023 [67,68].
Messenger RNA vaccines
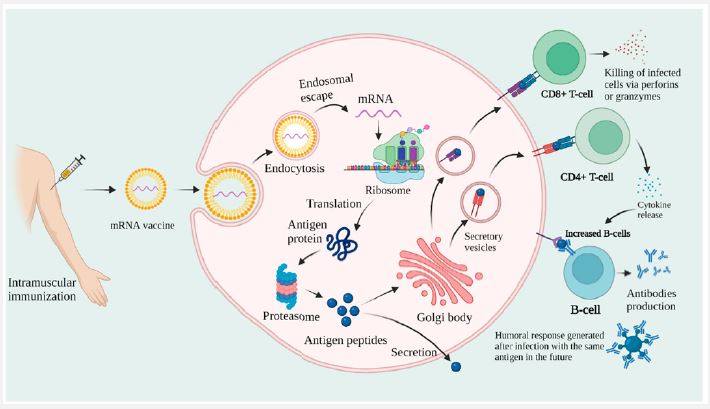
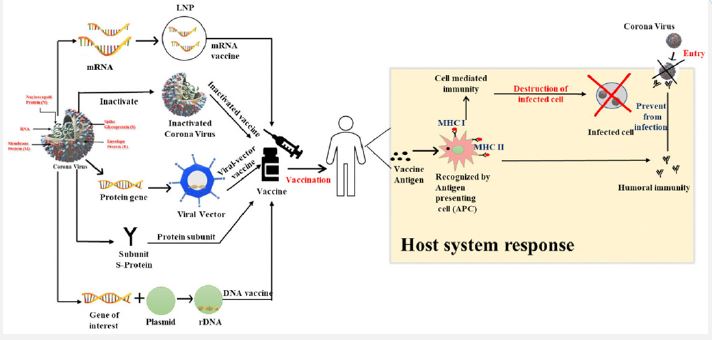
The concept behind mRNA vaccines involves introducing mRNA that encodes a viral protein into the host immune system to serve as an antigen, thereby stimulating an immune response and producing neutralizing antibodies. This approach differs fundamentally from traditional vaccines, which typically use inactivated pathogens or protein antigens to elicit immunity [65]. To create the mRNA, an RNA polymerase transcribes it in vitro from a DNA template containing an Open Reading Frame (ORF) that encodes the target protein. Once inside the host, the mRNA leverages the host’s translational machinery to synthesize the antigenic protein [23].
mRNA-based vaccines offer several advantages, including their relative safety, reliance on the host’s translational machinery, avoidance of genome integration, and the simplicity and scalability of production in laboratory settings. However, challenges such as efficient delivery, maintaining mRNA stability within the host, the potential for unintended immune responses, and storage limitations—requiring freezing to prevent degradation—remain significant hurdles. Despite these obstacles, mRNA vaccines are recognized as the fastest and most effective approach for developing a COVID-19 vaccine, positioning them as one of the most promising solutions for combating the pandemic [70,81].
The spike(S) protein of SARS-CoV-2 has considerable resemblance to the S protein of SARS-CoV, making it a crucial target for RNA vaccine development. This resemblance allows researchers to use established understanding about the S protein to develop viable vaccines for SARS-CoV-2. Neutralizing antibodies directed against the Receptor-Binding Domain (RBD) and the N-terminal domain of the S protein have been detected in a subset of COVID-19 patients, underscoring the potential of the S protein as an antigen and designating these domains as viable targets for vaccine development [24].
RNA vaccines that encode the spike (S) protein are an effective strategy for inducing neutralizing antibodies, which block the virus from binding to the ACE2 receptor and prevent its entry into host cells. However, this approach assumes that SARS-CoV-2 relies solely on ACE2 for cellular entry, leaving a potential vulnerability if alternative entry mechanisms exist. Additional technical challenges include ensuring the stability of the mRNA, its efficient uptake by host cells, and its successful release from encapsulating nanoparticles into the cytoplasm to produce the desired protein. Strategies to enhance mRNA stability often involve protecting it from degradation by host ribonucleases. The mRNA is typically delivered intramuscularly, encapsulated in lipid nanoparticles or similar materials, to ensure effective delivery and stability [25-27].
The mRNA-1273 vaccine, which contains modified viral RNA encapsulated in lipid nanoparticles, was the first mRNA vaccine developed to fight COVID-19. In a Phase 1 trial (NCT04283461), all participants developed neutralizing antibodies following administration of the vaccine, which encodes the stabilized prefusion spike(S) protein. The vaccine requires two doses. However, a considerable number of recipients experienced mild COVID-19-like symptoms as side effects. Since the immunogenicity triggered by mRNA vaccines is temporary, multiple doses are typically necessary to produce a strong and lasting immune response. One promising approach to overcome this limitation is the use of Self-Amplifying mRNA (SAM) constructs, which utilize a replicase to facilitate continuous transcription of viral mRNA, leading to sustained antigen presentation to the immune system.
The SAM strategy allows for the production of a large amount of antigen from a relatively small amount of mRNA. However, the SAM platform faces challenges due to the size limitations of the antigen inserts. Additionally, novel RNA constructs have been developed to maintain persistent antigen expression after a single injection, with one construct encoding the replicase and the other the target antigen. Moreover, transfecting dendritic cells with viral RNA has been shown to induce strong immune responses by activating T cells specific to the antigen [28,29].
Finally, nucleoside-modified mRNA vaccines have proven to be highly effective in presenting antigens and triggering an immune response. Many academic institutions and industry players are actively working to develop mRNA-based vaccines, employing a range of strategies based on the potential effectiveness of this technology. The safety and immunogenicity of several mRNA vaccines, including their ability to generate neutralizing antibodies, have already been assessed in Phase 1 and Phase 2 clinical trials. Large-scale Phase 3 trials assessing the efficacy of these vaccines have also begun enrolling participants [30].
DNA based vaccines
The approach involves transferring a SARS-CoV-2 gene, typically encoding the spike(S) protein, to induce an immune response through the expression of the viral protein. This is achieved using various vectors, such as plasmids, replication-competent vesicular stomatitis virus, replication-deficient adenoviruses, or lentiviruses. DNA vaccines offer several advantages, including stability at room temperature, good safety profiles, and ease of large-scale production at an affordable cost. These vaccines can be administered through methods such as electroporation, intramuscular injection, or intradermal injection. DNA vaccines have been developed for several infectious diseases and have demonstrated both immunogenicity and favorable safety profiles [42,43].
Investigations are underway to evaluate the immunogenicity and safety of DNA vaccines targeting SARS-CoV-2. Initial research in rhesus macaques has shown that the expression of numerous viral S protein immunogens elicits both humoral and cellular immunological responses, including the generation of neutralizing antibodies and the activation of CD4+ and CD8+ T cells that secrete IFN-g. In response to the SARS-CoV-2 virus, the DNA vaccination markedly decreased viral RNA levels, indicating a robust immune response [32,33]. Vaccinated individuals had dose-dependent antibody and T cell responses, with maximal responses seen about 4 weeks post-vaccination using a recombinant adenovirus that expresses the full-length S protein. Mild to severe side effects were prevalent, although no significant adverse events were documented, and a phase 2 trial of this vaccine has been completed. It is crucial to acknowledge that replication-deficient adenoviruses are immunogenic and might provoke host immunological responses that hinder transgene expression, presenting a hurdle in the first stages of gene therapy [31].
Protein based vaccines: Protein subunits, Virus-Like Particles (VLP) and peptides
Subunit vaccines consist of specific proteins or polysaccharides that are either extracted from natural sources or produced using recombinant DNA technology. These vaccines focus on selected viral antigens, which minimizes the risk of adverse reactions, though it remains essential to identify the most immunogenic antigenic components (Clem, 2011). One example is NVX-CoV2373, a subunit vaccine developed by Novavax, which includes the S protein and the Matrix-M1 adjuvant. Currently in phase III trials, NVX-CoV2373 has shown promise in preclinical and clinical studies [35,36].
Virus-Like Particles (VLPs) consist of the envelope and/or capsid proteins from various viruses, but they do not contain any genetic material. Although their production can be difficult, VLPs offer the advantage of mimicking the virus’s structure and antigenicity while being non-infectious. Medicago Inc. has developed a VLP-based vaccine, which is the only one to reach phase I clinical trials. This vaccine is plant-derived, using living plants as bioreactors to produce non-infectious virus-like strains and is adjuvanted to enhance the immune response (Medicago, 2021) [36,38].
Virus-Based vaccines include weekened or inactivated viruses
a. Weakened virus
Attenuated vaccines, using weaker variants of the pathogen, elicit robust humoral and cellular immune responses (Chen et al. 2020). These vaccinations often provide long-lasting protection with just a few numbers of doses. Nonetheless, their primary drawback is the possible hazard presented by the living microorganisms, which might, on infrequent occasions, return to their former, more aggressive state [38].
b. Inactivated virus
Chemical or physical methods are employed to inactivate pathogens, ensuring the vaccine’s stability. However, these vaccines often trigger a relatively weak immune response, necessitating multiple doses for optimal efficacy (Clem, 2011; Xia et al., 2020). Sinovac is conducting clinical trials on COVID-19 using various inactivated virus vaccines, including PiCoVacc. This vaccine has shown the ability to generate SARS-CoV-2-specific neutralizing antibodies in multiple preclinical models, such as mice, rats, and nonhuman primates (Gao et al. 2020). It has also demonstrated a favorable safety and immunogenicity profile in phase I/II trials, with phase III trials currently in progress [40,41].
Viral vectors vaccines
Utilize altered and non-related viruses that express one or more antigens. This method employs either living vectors, which are often attenuated, or non-replicating vectors. Adenovirus, measles virus, and Vesicular Stomatitis Virus (VSV) are among the most often used viral vectors (Rauch et al., 2018) [39]. The Ad5 vectored COVID-19 vaccine demonstrated substantial immunogenicity and tolerability in phase I trials (Zhu FC et al. 2020). Additionally, various phase III COVID-19 vaccines utilize adenoviral vectors that express the S glycoprotein, such as ChAdOx1, which yielded significant outcomes regarding T-cell response and neutralizing antibody generation (Folegatti et al. 2020) [44].
Status of vaccines
Status of various vaccines under development/ investigation for the Novel Coronavirus
| S. No | Vaccine candidates | Technology | Manufacturers/Sponsors/Trials location | Generic name | Ref |
|---|---|---|---|---|---|
| 1 | mRNA-1273, The Moderna vaccine | mRNA-containing lipidnanoparticle dispersion | BARDA (U.S.), NIAID, and Moderna | The COVID- 19Moderna Vaccine | [63] |
| 2 | BNT162b2 | mRNA | Fosun Pharma, Pfizer, and BioNTech (Germany, U.S.) | Tozinameran | [53] |
| 3 | (ChAdOx1 nCoV-19) or Astra- Zeneca(AZD1222) (Vaxzevria, Covishield) | Adenovirus vector modified in chimpanzees (ChAdOx1) | Oxford University, AstraZeneca (United Kingdom) | AstraZeneca The COVID-19 vaccine | [44] |
| 4 | Vac Gam-COVID (Sputnik V)) | Non-replicating vector for viruses | Russian Gamaleya Research Institute | COVID-Vac Gam | [76] |
| 5 | Convidecia (Ad5- nCOV) | Vector of recombinant adenovi-rus type 5 | Beijing Institute of Biotechnology, CanSinoBIO(China, Russia) | Ad5-nCOV | [5] |
| 6 | BBV152 (Covaxin) | The SARS-CoV-2 inactivated | Bharat Biotech, ICMR (India) | BBV152 | [79] |
| 7 | Ad26.COV2(JNJ-78436735; Ad26.COV2.S) | Non-replicating vector of infec- tion | Janssen Vaccines, Belgium, U.S, Brazil, SouthAfrica | Ad26.COV2 | [33] |
| 8 | NVX-CoV2373(Novavax, TAK-019) | Recombinant spike protein nanoparticle with adjuvant | Novavax, Serum Institute of India, Takeda Pharmaceutical (U.K, Japan) | SARS-CoV-2 Vaccine | [49] |
| 9 | CoronaVac | Inactivated SARS-CoV-2 | Sinovac Biotech (China, Brazil, Indonesia) | COVID-19Vaccine (Vero Cell) | [33] |
| 10 | BBIBP-CorV Sinopharm | The SARS-CoV-2 inactivated | China, Argentina, and the United Arab Emirates' Beijing Institute of BiologicalProducts. | Vero Cell, a Sino- pharm COVID-19 vaccine | [26] |
| 11 | EpiVacCorona | Peptide vaccine | Virology and Biotechnology State Research Center (Russia) | The EpiVakKorona | [27] |
| 12 | CoviVac | The Inactivated vaccine | Russian Chumakov Federal Scientific Center | The ChumakovCOVID-19 virus | [27] |
| 13 | ZF2001 (ZIFIVAX) | Vaccine recombinant for virus | Chinese Academy of Sciences (China) ZhifeiLongcom Biopharmaceutical | Dimer RBD | [24] |
| 14 | ARCoV | vaccine based on mRNA | Abogen Biosciences Co. and WalvaxBiotechnology Co. (China) | The COVID- 19vaccine, Walvax | [24] |
| 15 | ZyCoV-D | Plasmid DNA vaccine | India's Zydus Biotech | The ZyCoV-D | [33] |
| 16 | Abdala (CIGB 66) | Vaccine using protein subunits | Center for Biotechnology and Genetic Engineering(Cuba) | Unknown | [65] |
| 17 | VLA2001 | Vaccine that has been inactivated | National Institute for Health Research, Valneva(France, UK) | Vaccine for ValnevaCOVID-19 | [41] |
| 18 | CVnCoV (CureVac) | mRNA-based vaccine | Curevac, GSK (Austria) | CVnCoV | [23] |
| 19 | BacillusCalmette-Guerin (BCG) vaccine | Live-attenuated vaccine | University of Melbourne, Radboud University (Australia, Netherlands) | BCG Vaccine | [5] |
| 20 | INOVIO-4800 | Plasmid DNA vaccine | U.S.-based Inovio Pharmaceuticals | COVID-19Inovio Vaccine | [23] |
| 21 | COVAXX UB-612 | vaccination based on multitope peptides | Brazil's Vaxxinity United Biomedical Inc. | Covid-19 UB- 612 | [39]. |
| 22 | Gorrilla Adenovirus GRAd- COV2 | vaccine based on adenovirus | Leukocare, Univercells (Italy), and ReiThera | GRAd-COV2 | [39] |
| 23 | Trimer vaccine SCB-2019 | Vaccine using protein subunits | Sanofi, Clover Biopharmaceuticals, and GlaxoSmithKline (Australia) | SCB- 2019 | [67] |
| 24 | V-01 | vaccine made of recombinant proteins | Center for Disease Prevention and Control in GuangdongProvince, China | COVID-19 VaccineV-01 | [5] |
| 25 | Razi Cov Pars | Spike protein-based recombinant vaccination | Iran's Razi Vaccine Institute | Unknown | [41] |
| 26 | Nanocovax | Recombinant vaccine (Spike protein) | Vietnam's Military Medical Academy, Nanogen Biopharmaceutical | Unknown | [39] |
| 27 | Soberana 1 and 2 | Conjugated/monovalent vaccine | Finlay Institute of Vaccines (Cuba) | FINLAY-FR-1, FINLAY-FR-2 | [41] |
| 28 | AdCLD- CoV19 | vaccine based on adenovirus | Cellid, LG Chem (Korea) | AdCLD-COVID19 Vaccine | [67] |
| 29 | KD- 414 | vaccine that has been inactivated | Japan Agency for Medical Research and Develop- ment, KM Biologics | Unknown | [39] |
| 30 | VBI- 2902a | vaccine with virus-like particles(enveloped) | VBI Vaccines Inc. (U.S) | Unknown | [41] |
| 31 | COVID-eVax | Plasmid DNA vaccine | Takis, Rottapharm Biotech (Italy) | Unknown | [23] |
| 32 | S-268019 | vaccine made of recombinant proteins | Agency for Medical Research and Development ofJapan; Shionogi & Co., Ltd. | Unknown | [67] |
| 33 | GLS-5310 | Plasmid-based DNA vaccine | Korea's GeneOne Life Science, Inc. | Unknown | [65] |
| 34 | Covigenix VAX-001 | Plasmid-based DNA vaccine | Aegis Life, Inc. and Entos Pharmaceuticals Inc.(Canada) | Unknown | [67] |
| 35 | EXG-5003 | Intradermal vaccine candidate | Fujita Health University, Elixirgen Therapeutics,Inc. (Japan) | Elixirgen (EXG- 5003) | [66] |
| 36 | AKS-452 | Vaccine using protein subunits | Netherlands: Akston Biosciences, University Medi- cal Center Groningen | Unknown | [40] |
| 37 | DS-5670a | Recombinant protein vaccine | Dong-A Pharmaceutical, Korea Institute of Scienceand Technology | Unknown | [23] |
| 38. | ABNCoV2 | vaccine based on cVLP | Nordic A/S Bavarian ExpreS2ion Biotech | IMVANEX® | [24] |
| 39. | EuCorVac-19 | vaccine using nanoparticles | EuBiologics; Hospital of Eunpyeong St. Mary's | Unknown | [23] |
| 40. | Mambisa (CIGB 669) | Vaccine using protein subunits | Genetic Engineering and Biotechnology Center | CIGB 669 Mambisa | [76] |
| 41. | IIBR- 100 | vaccine against the recombinantvesicular stomatitis virus (rVSV) | Hadassah Medical Center, Sheba Medical Center Hospital,and Israel Institute for Biological Re- search | Brilife | [24] |
| 42. | AG0301-COVID19 | DNA vaccine | Agency for Medical Research and Development ofJapan; AnGes, Inc. | AG0301-COVID19 | [76] |
| 43. | GX-19N | DNA vaccine | Genexine | Unknown | [33] |
| 44. | LUNAR VACCINE (CoV19) | RNA vaccination that replicatesitself | Duke-NUS Medical School and Arcturus Thera- peutics | LUNAR-COV19 | [53] |
| 45. | MCTI-CIMATEC- HDT Vaccine | The RNA vaccine | GennovaBiopharmaceuticals, HDT Bio Corp, the National Institutes of Health, and the University of Washington | HGCO19 | [40] |
| 46. | MRT5500 | mRNA-based vaccine | Sanofi; Translate Bio | Unknown | [53] |
| 47. | AV-COVID-19 | vaccine using dendritic cells. | Dr. Kariadi's residence; Aivita Biomedical, Inc. | AV-COVID-19 | [24] |
| 48. | FAKHRAVAC (MIVAC) | Based on Inactivated vaccines | Research Center for Stem Cell Technology; Fakhra Clinical Trial Center; DefensiveInnovation and Research Organization | Unknown | [49] |
| 49. | NBP2001 | vaccine made of recombinant proteins | Seoul National University Bundang Hospital; Seoul National University Hospital; SK Bioscience Co., Ltd. | Unknown | [40] |
| 50. | SpFN | vaccine using spike ferritin nanoparticles | WalterReed Army Institute of Research; United States Army Medical Research and Development Command. | Unknown | [33] |
| 51. | KBP-201 | Vaccine using protein subunits | Velocity Clinical Research, PMG Research of Winston-Salem, ICON, DM Clinical Research, and Kentucky BioProcessing, Inc. | COVID-19 KBP | [49] |
| 52. | MEISSA MV-014-212 Vaccine | Recombinant live Intranasal vaccines | Meridian Clinical Research; Johnson County Clin- Trials; MeissaVaccines, Inc. | Unknown | [24] |
| 53. | BRAD -T PTX COV19- B | vaccine based on mRNA | The Canadian government and ProvidenceTherapeutics | Unknown | [33] |
| 54. | AdimrSC- 2F | vaccine using protein subunits | Ad Immune | AdimrSC-2f | [23] |
| 55. | bacTRL-Spike vaccine | Bifidobacteria-based monovalent oral vaccination | Symvivo Company | Spike BacTRL | [41] |
| 56. | COVAXX-19 | Immunization with monovalentrecombinant proteins | Royal Adelaide Hospital; CinnaGen; Vaccine Pty Ltd. | Covax-19™ | [33] |
| 57. | 2019-nCoV-RBD-OPT1 DelNS1 | The viral vector that replicates | Jiangsu Provincial Center for Disease Control and Prevention, Beijing Wantai BiologicalPharmacy, and Xiamen University | As of 2019, DelNS1-nCoV-RBD- OPT1 | [41] |
| 58. | V451UQ- CSL | vaccine using protein subunits | University of Queensland (CSL) | Sclamping SARS-CoV-2 | [49] |
| 59. | CoV2-1 VXA | Adenovirus type 5 vector recom- binant vaccine | Vaxart company | The VXA-CoV2- 1 | [24] |
| 60. | Ad-COVID | vaccine administered intranasally | Summit Biosciences, Altimmune, and the Univer- sity of Alabama atBirmingham | Unknown | [26] |
| 61. | COVAC-2 | Based on Protein subunit vac- cines | Vaccine and Infectious Disease Organization- International Vaccine Center; Universityof Saskatchewan | Unknown | [40] |
| 62. | AAVCOVID | vaccine based on genes | University of Pennsylvania; Massachusetts Eye and Ear; Massachusetts General Hospital | Unknown | [49] |
| 63. | SARS-CoV-2-S-ChAd | vaccine based on adenovirus | St. Louis's Washington University School ofMedicine | SARS-ChAd-CoV- 2-S | [40] |
| 64. | HaloVax Vccine | Vaccine that assembles itself | MGH Vaccine and Immunotherapy Center; Hoth Therapeutics,Inc.; Voltron Therapeutics, Inc. | HaloVax trademark | [26] |
| 65. | LineaDNA | DNA vaccine | Takis Biotech | Linear DNA Vaccine | [53] |
| 66. | PittCoVacc | Microneedle array recombinant protein subunitvaccine | School of Medicine at the University of Pittsburgh(UPMC) | Unknown | [76] |
| 67. | T-COVID™ | Intranasal vaccine | Autoimmune | Unknown | [53] |
| 68. | LNP-nCoVsaRNA | The RNA vaccine that amplifiesitself | Imperial College London | Unknown | [24] |
| 69. | V590 | Vesicular stomatitis virus recom- binant vaccine | Merck; IAVI | Unknown | [49] |
Status of these vaccines during different phases of clinical trials
a. Preclinical phase
• In vitro testing and animal models to evaluate safety and immunogenicity.
• Variant-specific new-generation mRNA vaccines.
• Innovative delivery techniques (electroporation for DNA vaccines, nanoparticles) [46,47].
b. Phase I: Safety and dose escalation
• Evaluate the initial immune response, safety, and tolerability in small groups (20-100 participants)
• mRNA vaccines: Moderna’s mRNA-1273 started in Phase I in March 2020.
• Inactivated vaccines: Early trials of Sinopharm and Sinovac [72,73].
c. Phase II: Immunogenicity and dosage optimization
• Verify immunological response, adjust dosage, and assess immediate safety in larger cohorts (hundreds of participants).[45]
• Novavax (NVX-CoV2373): Showed strong immune responses with adjuvant in Phase II trials.
• ZyCoV-D: DNA vaccine by Zydus Cadila demonstrated safety and immunogenicity in Phase II [74].
d. Phase III: Large-scale efficacy trials
• Evaluate efficacy and rare side effects across diverse populations (thousands of participants).
• Pfizer-BioNTech (BNT162b2): Completed Phase III with >95% efficacy against symptomatic COVID-19.
• AstraZeneca (ChAdOx1-S): Reported ~70% efficacy, varying with dosing regimens.
• Johnson & Johnson (Ad26.COV2.S): Demonstrated 66% efficacy against moderate to severe disease in Phase III [48,49].
e. Post-approval (Phase IV): Long-term monitoring
• Assess long-term safety and effectiveness in real-world setting.
1. Booster studies: Pfizer and Moderna evaluating third and bivalent doses against Omicron and other variants.
2. Mix-and-Match trials: Research into heterologous vaccine schedules (e.g., AstraZeneca followed by mRNA vaccines) [74,75,76].
| Vaccine Platform | Vaccine Name(s) | Phase I | Phase II | Phase III | Post-Approval Studies |
|---|---|---|---|---|---|
| mRNA | Pfizer-BioNTech, Moderna | Completed | Completed | Completed; high efficacy | Boosters, variant updates |
| Viral Vector | AstraZeneca, Sputnik V | Completed | Completed | Efficacy varies (70%-91.6%) | Real-world effectiveness |
| Protein Subunit | Novavax | Completed | Completed | ~90% efficacy | Pending wider approval |
| Inactivated Virus | Sinopharm, Sinovac | Completed | Completed | Efficacy 50%-79% | Global usage monitoring |
| DNA | ZyCoV-D | Completed | Completed | ~66% efficacy in Phase III | Early rollout |
Outcomes of these trials if any during the completion of the study/interim analysis
1. Interim analyses
• In order to help inform public health decisions and emergency use authorizations, interim analyses are carried out throughout a trial to evaluate initial safety and efficacy.
2. Outcomes of completed studies
• During trials, vaccines demonstrated good overall safety profiles, with the majority of side effects (such as fever, fatigue, and injection site pain) being mild to moderate.
• Although they were discovered after the product was put on the market, rare side effects like myocarditis (mRNA vaccines) and thrombosis (AstraZeneca, Johnson & Johnson) are still extremely uncommon [76].
| Vaccine name | Platform | Interim efficacyresults | Final outcomes | Real-world effectiveness | Notable findings |
|---|---|---|---|---|---|
| Pfizer-BioNTech | mRNA | 95% efficacy (PhaseIII) | Confirmed 95% efficacy; mild to moderateside effects | High protection against severe dis- ease; reduced efficacy for Omicron | Approved globally; recommendedboosters for waning immunity |
| Moderna | mRNA | 94% efficacy (PhaseIII) | Similar to Pfizer; strong protection against severe disease | Similar real-world effectiveness as Pfizer | Long-lasting T-cell response; booster doses effective |
| AstraZeneca | Viral vector | ~70% efficacy(varies by dose) | Effective but lower efficacythan mRNA vaccines | ~70% effective in real-world stud- ies; significant in low-resource settings | Rare blood clotting cases observed |
| Johnson & Johnson | Viral vector | 66% efficacy (PhaseIII) | 85% effective againstsevere disease;one-dose regimen | Effective against severe disease; lowerefficacy vs variants | Single-dose convenience for low- resource areas |
| Novavax | Protein subunit | 90% efficacy overall | Effective against Alpha; reduced efficacy for Beta | Pending real-world data; likelysimilar to trial results | Adjuvant boosts immune responsesignificantly |
| Sinopharm | Inactivated virus | ~79% efficacy(Phase III) | Safe and effective; efficacylower than mRNA vaccines | Effective at preventing severe disease; used widely in LMICs | Lower immunogenicity in elderly;booster shots recommended |
| Sinovac | Inactivated virus | ~50%-78% efficacy(varied by trial) | Effective but less robust im- mune response than others | Moderate real-world efficacy; good safety profile | Widely used; key in global vaccina- tion campaigns |
| Sputnik V | Viral vector (heterologous) | ~91.6% efficacy(Phase III) | High efficacy and protectionagainst severe disease | Effective in real-world studies; widely used in some regions | Two different adenoviral vectors reduceresistance risks |
| ZyCoV-D | DNA | ~66% efficacy(Phase III) | Safe and effective; first ap- proved DNA vaccine | Early data promising; pendingbroader real-world analysis | Needle-free delivery technology (jet injector) |
Various adverse effects related to the vaccines during these trials
1. Mild-to-Moderate effects:
• All vaccines frequently resulted in temporary systemic and local side effects, including fever, exhaustion, and injection site pain. Usually, these effects were self-limiting [57,58].
2. Serious adverse events:
• There was a slight risk of myocarditis with mRNA vaccines, particularly in younger males.
• Very uncommon cases of TTS and GBS have been linked to viral vector vaccines (AstraZeneca and Johnson & Johnson).
• Inactivated vaccines had the mildest profiles overall, while other platforms displayed fewer systemic or uncommon side effects [52-54].
Post-trial monitoring insights
• Rare adverse effects were detected by enhanced pharmacovigilance, guaranteeing continued safety;
• Booster doses were generally well-tolerated, with no appreciable rise in rare adverse events.
Risk-benefit ratio
• For all vaccines, the advantages of vaccination (such as preventing serious illness, hospitalization, and death) greatly exceeded the risks, even in the case of uncommon side effects [78-80].
| Vaccine Name | Platform | Common Adverse Effects | Rare Adverse Effects | Severity and Frequency | Post-Trial Monitoring Insights |
|---|---|---|---|---|---|
| Pfizer-BioNTech | mRNA | Fatigue,fever, headache,injection site pain | Myocarditis (more in younger males, 1:50,000), anaphylaxis | Mild to moderate; rare AEs very infrequent | Booster doses well- toleratedwith similar AE profile |
| Moderna | mRNA | Fatigue, chills, headache, injection site pain | Myocarditis (younger males), anaphylaxis | Slightly higher rates of sys-temic AEs vs Pfizer | Similarsafety for boosters; myocarditis cases manageable |
| AstraZeneca | Viral vector | Fatigue, fever, injection sitepain, muscle aches | Thrombosis with thrombocytope- nia syndrome (TTS), Guillain-Barré Syndrome | Very rare TTS (~1:100,000);higher in younger women | Risk-benefit ratio favorable, with continued usage |
| Johnson &Johnson | Viral vector | Fatigue, fever, injection sitepain, headache | TTS, Guillain-Barré Syndrome | Rare TTS (~1:500,000); lower frequency vs AstraZeneca | Safety monitoring led to tar- geted age-group advisories |
| Novavax | Protein subunit | Fatigue,fever, headache,injection site reactions | Myocarditis (rare), hypersensitivity reactions | Lower systemic AEs com- pared to mRNA vaccines | Awaiting real-world AE data; promising safety profile |
| Sinopharm | Inactivated virus | Injection site pain, fatigue,headache, fever | Rare allergic reactions | Generally mild and less frequent systemic AEs | High safety in real- worldstudies, including elderly |
| Sinovac | Inactivated virus | Injection site pain, fatigue,headache, fever | Rare allergic reactions | Lower rate of AEs vs mRNAand viral vector vaccines | Similar safety profile globally |
| Sputnik V | Viral vector | Fatigue, fever, headache, muscle pain | No notable rare AEs reported | Mild to moderate AEs; goodtolerability | Long-term safety data limited |
| ZyCoV-D | DNA | Fatigue,fever, headache,injection site redness | No major rare AEs reported | Mild AEs; injection site reac- tions common | Needle-free delivery reducedinjection pain |
In addition to being effective at preventing serious illness and death, the COVID-19 vaccines are anticipated to offer at least some protection against novel virus variants [61]. This is due to the fact that these vaccines elicit a wide-ranging immune response, so any modifications or mutations in the virus shouldn’t render them totally ineffective. It will be feasible to alter the vaccines’ composition to provide protection against these variants if any of them lose their effectiveness against one or more of them. Data on novel COVID-19 virus variations is still being gathered and examined.
In order to prevent mutations that could lessen the effectiveness of current vaccines, we must take all reasonable steps to stop the virus’s spread while we learn more. This entails keeping a minimum of one meter between you and other people, covering your elbow when you cough or sneeze, washing your hands often, donning a mask, avoiding poorly ventilated spaces, and opening windows.
The baseline effectiveness of a COVID-19 vaccine had a significant impact on its acceptance. It might be challenging to get the general public to accept a vaccine with comparatively low efficacy [55,56].
Therefore, creating a COVID-19 vaccine that is suitable for use everywhere is a top priority. The process of developing a vaccine is time-consuming and costly [59,60]. Preclinical testing concurrent with phase 1 clinical trials, platform development, and simple licensing are some of the new strategies that have been introduced to speed up the development of an appropriate COVID-19 vaccine. Gaining more knowledge about SARS-CoV-2’s traits can aid in directing the creation of more targeted vaccinations. 115 of the more than 200 vaccine candidates that have been reported so far have advanced to phase 1, 2, or even 3 clinical trials. A COVID-19 vaccine’s demonstrated safety and effectiveness are crucial factors to take into account before approving it. To guarantee that everyone has equal access to resources, careful and comprehensive planning must. Priority should be given to administering vaccines to high-risk individuals and medical personnel. Issues pertaining to supply chains, ownership of vaccines, and funding large-scale production need to be fixed [62,63].
Acknowledgments: We received a lot of help from several people to complete this review.
I extend my gratitude to School of Pharmaceutical Education and Research Jamia Hamdard New Delhi-110062, School of Pharmaceutical Sciences Glocal University Mirzapur Pole Saharanpur 247121, Department of Research and Development, AIMIL Pharmaceuticals, New Delhi, India who provided us with the required facilities.
Funding source: No funding was received for this project.
Conflict of interest: The authors declare no competing interests.
Data availability: All authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Author contributions: Conceptualization-K.D, M.K.; Data curation-K.D., M.K., S.A; Project Administration-K.D, M.K., Z.K, S.A. Supervision-K.D, S.A; Visualization-M.K, Z.D.K.D; Writing — original draft-M.K.; Writing review & editing-K.D, M.K, Z.D., Z.K.
