Medical University of Warsaw, 61 Żwirki i Wigury Street, 02-091 Warsaw, Poland.
Mandalian Andrzej
Email: s078998@student.wum.edu.pl
Received : Feb 20, 2026 Accepted : Mar 24, 2026 Published : Mar 31, 2026 Archived : www.meddiscoveries.org
Type 2 Diabetes Mellitus (T2DM) represents a global health challenge. While Continuous Energy Restriction (CER) is the standard dietary intervention, it is often hindered by poor long term-adherence. Intermittent-Fasting (IF) and Time-Restricted Eating (TRE), a subtype of Intermittent-Fasting regimen and an intervention that tries to align food intake with circadian rhythm of the pancreatic beta cells, has emerged as an alternative.
The aim of this review is to evaluate the efficacy and safety of IF, with a specific emphasis on Time-Restricted Eating (TRE) as an adjunctive therapy for T2DM. This analysis focuses on recent evidence published between 2020 and 2025, highlighting the distinct circadian mechanisms of TRE compared to broader fasting protocols.
Recent randomized controlled trials indicate that IF and TRE significantly improve glycaemic control and promote weight loss comparable to that of Continuous Energy Restriction. TRE represents a safe and effective therapeutic strategy for T2DM. It offers synergistic benefits when combined with exercise and may facilitate the reduction of pharmacological treatment. It operates on mechanisms distinct from simple caloric restriction; aligning calorie intake with circadian rhythm and promoting “beta-cell rest”. TRE’s advantage over calorie-restricting diets lies in glycaemic stability. It significantly improves “Time in Range” (TIR) and reduces fasting glucose with weight loss being a secondary result of unintentional calorie reduction. Intermittent Fasting (e.g., 5:2, ADF) seems to drive results primarily through significant caloric deficits, leading to superior weight loss and HbA1c reduction compared to pharmacological treatment (e.g., Metformin).
Recent trials demonstrated that if appropriate protocol adjustments are made, then IF interventions could be safe options in managing T2DM
Keywords: Type 2 Diabetes; Time-restricted eating; Intermittent fasting; Circadian rhythm; Glycaemic control.
Type 2 Diabetes Mellitus (T2DM) is a chronic metabolic disease managed primarily through pharmacotherapy and lifestyle modification, including dietary intervention. While Continuous Energy Restriction remains the standard recommendation for glycaemic control and body weight management, it suffers from poor adherence to daily caloric restriction, which in time leads to weight gain and disease progression [1]. This poor adherence leads to growth in interest in alternative dietary strategies that may be simpler to implement and sustain.
Interventions focusing on meal timing rather than caloric restrictions have gained attention. Such interventions are collectively known as “Intermittent Fasting” (IF). Common IF strategies include Alternate-Day Fasting (ADF), the 5:2 diet (two days of severe energy restriction and 5 days of eating “ad libitum”), and Time-Restricted Eating (TRE) [2]. TRE involves consuming all daily energy intake within a specific time window and fasting for the remaining part of the day. TRE does not require daily calorie counting, which differentiates it from dietary interventions commonly associated with T2DM.
The physiological reason behind implementing TRE in T2DM is stemming from circadian biology. Modern eating patterns, characterized by high meal frequency and late-night consumption, lead to desynchronization of peripheral circadian clocks in the liver, adipose tissue, and pancreas, which all could contribute to insulin resistance [3]. Mechanistic studies suggest that extending the overnight fasting interval restores circadian alignment and enables “beta-cell rest” enhancing autophagic processes within pancreatic islets [4].
Despite the theoretical benefits, the clinical application of TRE in patients with T2DM still remains a subject of debate particularly due to concerns regarding the risk of hypoglycaemia in insulin-treated patients. Earlier clinical guidelines published before 2023 recommend against the use of IF in patients with T2DM due to lack of sufficient evidence [5]. These recommendations guidelines are challenged by emerging data from recent years that suggests that TRE may be both safer and more feasible than CER in the T2DM population, while providing similar metabolic outcomes.
The aim of this review is to synthesize current scientific evidence, regarding the efficacy and safety of TRE as an adjunctive strategy in T2DM. Our paper evaluates the influence of TRE on glycemic control. Glycemic control will be measured including metrics such as Time in Range [TIR], weight reduction, and potential for de-escalation of pharmacological treatment.
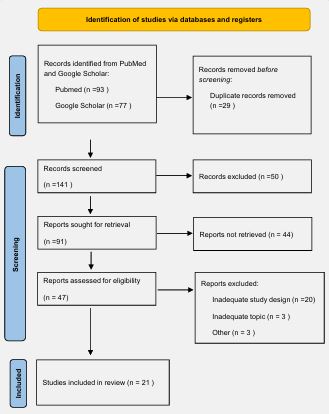
A comprehensive literature search was conducted in the PubMed database. Electronic literature searches were performed with a restriction to particular publication years (2020-2025). Studies were included if they involved either adults or the paediatric population with established T2DM undergoing IF protocols (including TRE) and reported on glycaemic control, insulin sensitivity, safety outcomes, weight loss or other metabolic outcomes. Data from clinical trials, systematic reviews, and original papers, as well as meta-analyses were considered and screened for relevance. Exclusion criteria, however, included studies with inadequate methodology and publications written in languages other than English. The exact number of included and excluded studies is illustrated in the PRISMA flowchart (Figure 1).
| Author (Year) | Study population | Intervention protocol | Key findings |
|---|---|---|---|
| Guo et al [1]. | Adults with T2DM | 5:2 Diet (Meal replacement) vs. Metformin vs. Empagliflozin | The 5:2 diet resulted in superior HbA1c reduction (-1.9%) compared to pharmacological treatments (-1.6% and -1.5%) and significant weight loss (-9.7 kg). |
| Obermayer et al [7]. | Insulin-treated T2DM patients | Intermittent Fasting (3 days/week) with 20% basal insulin reduction | Significant reduction in HbA1c (-0.73%) and body weight (-4.8 kg) without severe hypoglycemic events; enabled insulin dose reduction. |
| Sukkriang & Buranapin [8]. | Obese patients with T2DM | TRE 16:8 vs. TRE 14:10 (3 days/week) | Both protocols significantly reduced HbA1c. The 16:8 group achieved greater weight loss (-4.02%) compared to the 14:10 group (-3.15%). |
| Parr et al [9]. | Adults with T2DM | 9-hour TRE window vs. Standard Dietetic Advice | TRE resulted in HbA1c reductions comparable to standard care over 6 months; benefits were linked to weight loss rather than timing alone. |
| Hegedus et al [18]. | Adolescents with T2DM | Late TRE (12:00-20:00) | High adherence (6.2 days/week) and spontaneous caloric reduction (-271 kcal/day); demonstrated feasibility of later eating windows. |
| Bravo-Garcia et al [13]. | Adults with T2DM | 8-hour TRE + post-meal exercise | Combination of TRE and exercise significantly reduced insulin levels, suggesting a synergistic effect on insulin sensitivity. |
Hypothetical pathophysiological mechanisms: Beta-Cells and Circadian Rhythm.
Understanding the underlying mechanisms of TRE helps to distinguish it from interventions based solely on calorie reduction and different intermittent-fasting regimens. Current literature highlights the restoration of circadian rhythms as a key mechanism. Harris and Czaja note that contemporary eating patterns disrupt peripheral clocks in the pancreas and liver; TRE would realign nutrient intake with the body’s active phase improving metabolic flexibility [3]. This “circadian alignment” is supported by Parrotta et al., who describe how fasting intervals activate autophagy and reduce oxidative stress [6]. Brown and Matveyenko further propose the concept of “beta-cell rest”, suggesting that prolonged fasting periods could reduce the secretory demand on beta-cells, alleviate ER stress and preserve beta-cell mass and function [4]. This mechanistic theory aligns with clinical findings of improved beta-cell responsiveness observed in a trial of Msane et al., who noted the potential of TRE to reverse prediabetes progression [2].
Impact on glycaemic control and weight loss: Clinical targets in T2DM management are mainly glycaemic control and weight reduction. Recent Randomized Controlled Trials (RCTs) provide strong evidence for the efficacy of various intermittent fasting strategies, including TRE. A RCT by Guo et al. showed that a 5:2 meal replacement strategy was superior to pharmacological treatments; the intervention group achieved a greater HbA1c reduction (-1.9%) compared to patients on Metformin (-1.6%) and Empagliflozin (-1.5%), along with substantial weight loss (-9.7 kg) [1]. Obermayer et al. reported that in insulin-treated patients, an intermittent fasting protocol that lasted only 3 days per week reduced HbA1c by -0.73% and body weight by -4.8 kg, which enabled insulin dose reduction [7].
The evidence suggests efficacy of TRE is comparable to standard care, which is a calorie-restricting diet. Sukkriang & Buranapin showed that a flexible TRE schedule (fasting 14-16 hours for 3 days/week) significantly reduced HbA1c compared to controls [8]. Parr et al., found that a 9-hour TRE window resulted in HbA1c reductions comparable to standard dietetic guidance over six months [9]. Tricò et al. observed similar reduction in HbA1c in the early time-restricted Carbohydrate consumption group vs Mediterranean Diet group. There was no added metabolic benefit of early carbohydrate restriction over a calorie-matched Mediterranean diet [10].
Meta-analyses from Nam et al. highlighted that TRE specifically increases Time in Range [TIR] by +10.51% and reduces fasting glucose. It emphasizes its role in stabilizing daily fluctuations rather than just lowering average glycemia [11]. Meta-analysis by Samnani-Azad et al. indicated that while ADF showed a slight advantage over Continuous Energy Restriction (CER) for weight loss, daily TRE performed similarly to CER [12]. These findings suggest that periodic IF like 5:2 may drive results primarily through significant caloric deficits. TRE on the other hand primarily benefits glycaemic stability. Weight loss during TRE would be a derivative of spontaneous and unintentional calorie restriction.
Combining TRE with other lifestyle modifications may enhance therapeutic outcomes. Bravo-Garcia et al. conducted a randomized crossover trial examining the acute effects of combining an 8-hour TRE window (10:00-18:00) with post-meal exercise in patients with T2DM. TRE alone did not significantly alter the 14-hour glucose Area Under the Curve (AUC) compared to a 12-hour eating window. The combination of TRE and exercise significantly reduced insulin levels, suggesting a synergistic effect of combined exercise and TRE on insulin sensitivity [13].
Regarding the sustainability of metabolic benefits, a study by Ekberg et al. provided evidence supporting long term effects of the 5:2 diet. The significant reductions are HbA1c, body weight and weight circumference observed after the 6-month intervention were often maintained at the 12-month post intervention follow-up. The study also found persistent improvements in HOMA-IR, an index used to measure insulin resistance, suggesting that IF could produce lasting metabolic benefits [14].
For an overview of the key findings from the RCTs, particularly regarding glycaemic control and weight loss, please refer to (Figure 2).
Effects on lipid metabolism and cardiovascular risk: Glycemia is not the only metabolic parameter affected by TRE. In the INTERFAST-2 trial, Pammer et al. found that TRE did not improve HDL cholesterol more than a standard diet, it did however increase serum levels of apolipoprotein M (Apom). Apom is a marker linked to insulin sensitivity and lipid metabolism [15]. Kirkham et al. reviewed that TRE consistently reduces blood pressure and may improve lipid profiles; however, these changes are proportional to the weight that was lost [16]. A systematic review by Silva et al. highlights those metabolic effects of TRE intervention depend on the patient’s initial health status. The authors observed that IF regimens have major beneficial effects in the improvement of dysregulated metabolic conditions for obese individuals. The improvements are seen throughout adiposity, lipid homeostasis and blood pressure. The beneficial effects for patients with T2DM were less pronounced, but substantial in their major metabolic dysfunctions [17].
Timing and feasibility: Sukkriang & Buranapin demonstrated that intermittent TRE, practiced only 3 days per week, is sufficient to induce metabolic improvements. In their study, both 16:8 (16 hours fasting) and 14:10 protocols significantly reduced HbA1c compared to controls. The 16:8 regimen produced greater weight loss (-4.02% vs. -3.15%) [8], indicating that adhering to a narrower eating window does not need to correspond with more robust clinical benefits. This enhances the feasibility of a therapeutic intervention.
Regarding the timing of the eating window, Hegedus et al. conducted a “Late TRE” protocol (12:00-20:00) in adolescents with T2DM. This feasibility trial reported high adherence (6.2 days/week) and a spontaneous caloric reduction of -271 kcal/ day. It proved that shifting the window to later hours could be a strategy for specific populations who may struggle with early restricted feeding [18].
The safety profile of TRE concerning hypoglycaemia in patients treated with insulin or sulfonylureas, has been a subject of debate. In 2022, the Korean Diabetes Association issued a statement recommending against the use of intermittent fasting in patients with T2DM due to a lack of evidence and potential hypoglycaemia risks [5]. RCTs that emerged later challenge this recommendation.
A trial by Obermeyer et al. provides safety data for insulin treated patients [7]. A protocol of 20% basal insulin reduction was implemented on fasting days. A significant reduction in HbA1c and body weight was observed without the occurrence of severe hypoglycaemic events [7]. A systematic review by van den Burg et al. highlighted the potential of TRE for lowering the dose of oral antihyperglycemic agents. Across 13 reviewed studies, 4 reported a reduction in the dosage of glucose-lowering medication during the intervention [19]. This evidence suggests that with proper medication adjustment and monitoring, TRE is a feasible therapeutic option that may facilitate the de-escalation of pharmacological treatment.
Questions have been raised regarding the impact of time restricted feeding schedules on sleep quality. However, an analysis of a 6-month RCT by Pavlou et al. dispelled these concerns [20]. The study found that TRE (12:00-20:00) did not negatively affect sleep duration, quality, or insomnia severity compared to daily calorie restriction or a control group. These findings indicate that TRE does not compromise sleep in patients with T2DM [20].
The synthesized evidence presents TRE as a promising adjunctive therapy for T2DM. A central debate in the current literature is whether the metabolic benefits of TRE stem purely from spontaneous caloric restriction or from physiological alignment with circadian rhythms. Studies such as those by Parr et al. and Tricò et al. suggest that when control groups adhere to a rigorously matched caloric deficit, the specific advantage of TRE diminishes [9,10]. This supports the hypothesis implying that TRE is primarily a behavioural tool to facilitate energy deficit without the need of counting calories.
On the other hand, the meta-analysis by Nam et al. identifying significant improvements in TIR and the finding by Bravo-Garcia et al. regarding synergistic insulin lowering with exercise suggest metabolic benefits that are beyond weight loss [11,13]. These effects are likely mediated by the restoration of peripheral circadian clocks and the induction of “beta-cell rest,” mechanisms that reduce oxidative stress and preserve pancreatic function.
The 2022 consensus by Choi et al. issued a recommendation against IF in T2DM due to fears of hypoglycemia and lack of evidence [5]. In contrast, subsequent high-quality trials have demonstrated that TRE is safe even in insulin-treated patients if medication doses are adjusted (e.g., a 20% reduction in basal insulin on fasting days) [1,7]. This supports the view that TRE should no longer be viewed as contraindicated but rather as a supervised dietary strategy requiring clinical supervision, that may facilitate medication reduction, as noted by [19]. However, TRE has its limitations. Liu et al. found that the metabolic benefits of TRE are most powerful in the short term (< 3 months), and the long-term durability of these effects is uncertain [21].
Recent evidence points to the conclusion that IF and TRE are viable adjunctive therapies for Type 2 Diabetes Mellitus. 2022 guidelines against IF in T2DM recommending against IF in T2DM need to be re-evaluated. Recent trials demonstrated that if appropriate protocol adjustments are made, then IF interventions could be safe options in managing T2DM. Future clinical practice should focus on personalizing the implementation of eating windows to enhance long-term adherence.
Author’s contributions:
Andrzej Mandalian: Conceptualisation, methodology, formal analysis, investigation.
Andrzej Mandalian: Methodology, writing - original draft.
Maciej Malinowski: Formal analysis, writing - review & editing.
Natalia Żelichowska: Resources, data curation, writing - review & editing.
Katazyna Zadrożna: Resources, data curation.
Katarzyna Zadrożna: Visualisation.
All authors have read and agreed with the final, published version of the manuscript.
Acknowledgements: Not applicable.
Ethical approval: Not applicable.
Funding: This study has not received any external funding.
Conflict of interest: The authors declare no conflicts of interest.
Data and materials availability: All data sets collected during this study are available upon reasonable request from the corresponding author.
