Department of Integrative Biomedical Sciences, Faculty of Health Sciences, University of Cape Town, South Africa.
Chacha M Issarow
Email: chacha.issarow@uct.ac.za
Received : Mar 19, 2026 Accepted : Apr 22, 2026 Published : Apr 29, 2026 Archived : www.meddiscoveries.org
Background: The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is transmitted between humans through aerosols. It is assumed that protective face masks prevent the spread of SARS-CoV-2. However, face masks vary in their type and efficacy and the reported effectiveness of face masks to prevent the spread of SARS-CoV-2 has varied although the reason for this variation is not well understood.
Methods: In this study, a flexible mathematical model was developed and simulated under non- steady-state conditions to assess the impact of differing conditions and settings on the effectiveness of two types of face mask (low and high efficacy masks) in reducing SARS-CoV-2 transmission.
Results: This study found that spatial volume, the room ventilation as measured by Air Change/Hour (ACH), and duration of exposure were all important determinants of face mask protection effectiveness. Results in this study show that for a mask with a high efficacy of 95% (N95 respirators), the probability of acquiring a SARS-CoV-2 infection was high when room ventilation was limited (1 ACH) and low at 12 ACH. The same was true for a mask with a low efficacy of 40% (surgical face masks). This study found that for both the high and low efficacy face masks, the probability of acquiring SARS-CoV-2 infection was high in a space volume of 20 m3 and low in a space volume of 210 m3. Finally, it shows that for both types of masks, the probability of contracting SARS-CoV-2 infection was low after 100 minutes and high after 400 minutes of exposure. After 800 minutes of exposure, the probability of infection was approximately equal to 1 for all mask types (low and high efficacy masks).
Coclusion: Results in this study indicate that the effectiveness of a mask to prevent an aerosol infection like SARS-CoV-2 will depend both on the type of mask but also on the conditions and the settings. If exposure is short and distance between individuals can be maintained, even a low-efficacy mask may be protective, on the other hand, if exposure times are long in crowded spaces, then a highly effective mask such as a N95 respirator will be required for protection.
Keywords: Mask efficacy; Airborne virus; SARS-CoV-2; Mathematical model.
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) that causes COVID-19 is mainly transmitted between humans through aerosols [1,2]. Masks, including N95 respirators, surgical masks, and cloth masks, have been widely utilized to reduce inhalation exposure to SARS-CoV-2 [3-6]. In healthcare settings, N95 respirators and surgical masks are considered non-pharmacological means of preventing SARS CoV-2 transmission [7-10]. Many countries have mandated mask wearing in indoor public areas to curb the spread of SARS CoV-2. However, the use of masks to prevent the spread of SARS-CoV-2 is controversial and the reason why the protective effectiveness of similar masks, such as N95 respirators or surgical masks, varies in different reports is not well understood.
In this study, I developed and simulated a flexible mathematical model with varying room ventilation, space volumes, and duration of exposure to assess the effectiveness of high efficacy and low efficacy masks in reducing the spread of SARS-CoV-2 under non-steady-state conditions.
The aim of the study was to explore the effectiveness of masks, such as N95 respirators and surgical masks on reducing the spread of SARS-CoV-2. Let’s consider a susceptible individual wearing a mask who became exposed to an infectious individual in a confined space with limited ventilation as illustrated in Figure 1.
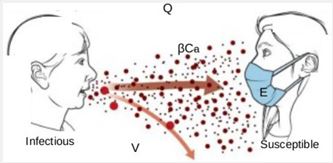
SARS-CoV-2 transmission in Figure 1 can be demonstrated mathematically as follows:

I=n−j, where I is an infectious individual, n is the total number of individuals in the given space, j is a number of susceptibles, V is space volume, β is expelled airborne infectious particles per unit time, Ca is a fraction of carbon dioxide in rebreathed air, C is the concentration of infectious particles, Q is the ventilation rate in the space and E is the mask efficiency or efficacy, computed as E=100%−µ, where µ is the penetration of particles through a certified mask. For example, efficiency of a certified N95 respirator is assumed to be 95%.
Arranging equation (1) and integrating from 0 to t, we obtain the concentration of infectious particles in the space at time t under non-steady state conditions:

Simplifying equation (2) further, we obtain the concentration of infectious particles expelled by infectious individual under non-steady-state conditions:

Where t is an exposure time in the given space.
Integrating equation (3) per(c̄) elapsed time, we obtain the average concentration ( individuals in the space:

Since not all infectious particles reach and deposit the alveolar to commence the infection, the average number of infectious particles inhaled by susceptibles that reach the infection site is determined by deposition fraction (θ). Thus, the average number of infectious particles (λ̄ ) that reach the alveolar to induce infection is equal to the product of the volume of breathed air (pt), deposition fraction and average concentration of infectious particles:

where p is a breathing rate.
Since the transmission of airborne respiratory infections, such as SARS-CoV-2 follows the Poisson distribution [16], we obtain an equation that predicts the risk of acquiring airborne infection in confined space under non-steady-state conditions as:

where P is the probability of acquiring airborne infection in the space, while the probability of not being infected is written as e−λ̅ . Substituting Equation (5) into Equation (6), we obtain an equation that predict the probability of acquiring airborne infection under non-steady-state condition when wearing a mask as:

Equation (7) was therefore simulated numerically with real-world values to assess the transmission probability of the causative agent of COVID-19, SARS-CoV-2 when wearing masks with varying mask efficiency in a space volume with different ventilation rates and duration of exposure.
| Parameters | Description | Value | Source |
|---|---|---|---|
| V | Space volume | 20 - 210 m³ | [11,14] |
| p | Breathing rate | 0.12 L/s | [11,16] |
| θ | Deposition fraction | 0.01 - 0.2 | [15,16] |
| I | Infectious individuals | 1-5 | Estimated |
| Ca | Fraction of carbon dioxide in rebreathed air | 0.04 | [11] |
| β | Infectious particles per unit time | 2 - 30 particle/s | [11,14] |
| t | Elapsed time | 0 - 1000 min | Estimated |
| E | Mask efficiency | 40 - 100% | Estimated |
| Q | Ventilation rate | 0 - 12 ACH | [11,16] |
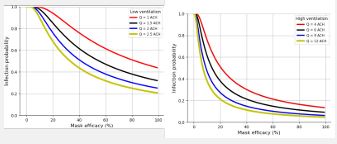
SARS-CoV-2 is typically spread via aerosol between individuals including in healthcare settings [11]. Model simulationin this study under non-steady state conditions with varying space volume, room ventilation, mask efficacy, and duration of exposure is presented in figures 2, 3, and 4. This study examined two types of masks with varying reported effectiveness: masks with a high efficacy of 95%, such as N95 respirators and a mask with a low efficacy of 40% (surgical face masks).
Room ventilation: For the high efficacy mask the probability of being infected with SARS-CoV-2 was 0.450 in a room with 1 Air Change/Hour (ACH), 0.260 at 2 ACH, 0.095 at 6 ACH, and 0.046 at 12 ACH (Figures 2a, and 2b). For the low efficacy mask, the probability of acquiring SARS-CoV-2 infection was 0.761 at 1 ACH, 0.509 at 2 ACH, 0.211 at 6 ACH, and 0.111 at 12 ACH.
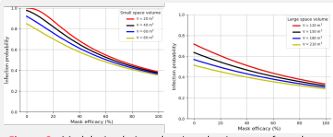
Space volume: This study found that for a high efficacy mask the probability of acquiring SARS- CoV-2 infection was 0.401 in a space volume of 20 m3, 0.377 in 60 m3, 0.322 in 150 m3, and 0.293 in a space volume of 210 m3 (Figures 3a, 3b). For a mask with a low efficacy, the probability of being infected was 0.685 in a space volume of 20 m3, 0.609 in 60 m3, 0.466 in 150 m3, and 0.398 in a space volume of 210 m3.
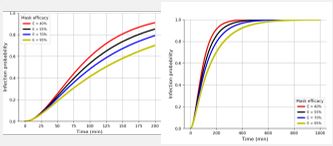
Duration of exposure: The risk of acquiring SARS-CoV-2 infection increases linearly with increasing duration of exposure (Figures 3a, 3b). For high efficacy masks, the probability of acquiring a SARS-CoV-2 infection was 0.417 in 100 min, 0.704 in 200 min and 0.926 in 400 min of exposure. For a mask with a low efficacy, the probability of being infected was 0.601 in 100 min, 0.915 in 200 min and 0.999 (≈1) in 400 min of exposure (Figures 4a, 4b). This study found that the probability of being infected was 0.999 (≈1) from ≥ 800 min of exposure in all mask types (low and high efficacy masks) (Figure 4b).
Results in this study indicate that face masks, even those with lower efficacy may reduce the likelihood of SARS-CoV-2 transmission to a vulnerable individual depending on how crowded, how well the room is ventilated, and the duration of exposure the individual has to an infectious environment.
On the other hand, even highly efficacious face masks may fail with prolonged periods of exposure to SARS-CoV-2 infectious aerosols accumulating in confined and poorly ventilated settings.
This study has shown why highly effective facial protection, such as N95 respirators, may equate to the level of protection of less effective protective face masks under certain conditions. If an N95 mask is used in a crowded space for long periods of time in a poorly ventilated room, then break through transmission may occur, whereas a surgical face mask may be highly effective where spatial volumes are large with high ventilation rates and periods of exposure are short.
These findings may help us interpret variation in reported studies. One study [17] reported that approximately 2% of Marine Corps recruits who tested negative for SARS-CoV-2 at the beginning of supervised quarantine that involved mask wear became positive by day 14. Confined living spaces with limited ventilation rates and a high duration of exposure among recruits during training, place military populations at high risk for contracting SARS-CoV-2. In other words, shared rooms with limited ventilation rates and prolonged platoon membership were important risk factors for SARS- CoV-2 transmission among recruits. Another study [18] reported that 1.8% of participants who were recommended to wear masks outside the home acquired the SARS-CoV-2 infection. It was reported that mask wearing recommendations to supplement other public health measures did not reduce the SARS-CoV-2 infection rate among wearers by more than 50% in a community with modest infection rates. This indicates that mask-wearing outside the home did not prevent SARS-CoV-2 infection for mask wearers in other settings, such as public transport and shops with limited ventilation and a high duration of exposure.
In contrast, one study [19] reported that during the intervention period of universal masking in healthcare settings, the positivity rate of SARS-CoV-2 infection decreased linearly from 14.65% to 11.46%, with an approximately daily decline of 0.49% among healthcare workers. Another study [20] reported that wearing masks all the time during contact, maintaining > 1 m distance from an infected individual, and having close contact for < 15 minutes were associated with a lower risk for SARS- CoV-2 infection. It shows that masks (even low-efficacy masks) become more effective in ventilated settings with short periods of exposure and if social distance between individuals can be maintained. Masks have played an important role, but it is important to consider the setting and conditions when thinking about the type of mask that will offer the best protection.
A randomized trial study [12] enrolled and randomly assigned the intervention to 446 nurses, of whom 225 received surgical masks and 221 received N95 respirators. The study aimed to compare the surgical mask with the N95 respirator in protecting health care workers against influenza. They found that influenza infection occurred in 50 nurses (23.6%) among surgical mask users and in 48 (22.9%) among N95 respirator users. The study concluded that the use of a surgical mask compared with an N95 respirator resulted in non-inferior rates of laboratory-confirmed influenza. One study [13] that reviewed the effectiveness of physical interventions to interrupt or reduce the spread of respiratory viruses reported that masks (surgical masks or N95 respirators) were the most consistent and comprehensive supportive intervention across populations and settings. However, N95 respirators were non-inferior to surgical masks but more expensive, uncomfortable, and irritating to the skin. The study could not find evidence that the more expensive, irritating, and uncomfortable N95 respirators were superior to surgical masks.
Competing interests: The author declares no competing interests.
